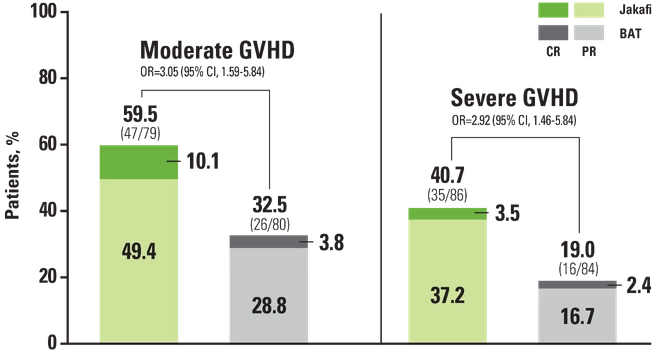
ORRs were higher with Jakafi® (ruxolitinib) regardless of disease severity1,2
REACH3 Subgroup Analysis: ORR by Baseline Disease Severity at Week 241,2


When managing our patients, we do not delay treatment. We take an aggressive approach and intervene with Jakafi at the first signs of initial treatment failure to not let cGVHD smolder over time.
Preet M. Chaudhary, MD, PhD GVHD Expert

REACH3 primary endpoint
REACH3 Primary Endpoint: ORR at Week 241,a

ORR Through Week 243,c

aORR was defined as the proportion of patients with CR or PR at week 24, according to 2014 NIH consensus criteria.1
bOne-sided P value, OR, and 95% CI were calculated using stratified Cochran-Mantel-Haenszel test, stratifying for moderate and severe cGVHD.1
cDefined as the proportion of patients who achieved CR or PR through week 24 (cycle 7, day 1), according to 2014 NIH consensus criteria.3
Patients treated with Jakafi were
3×
more likely to achieve an overall response at week 24 vs BAT (OR, 2.99)1
Median time to first response
3
weeks (range: 2-24) with Jakafi and 4 weeks (range: 2-25) with BAT2
- 74% of patients treated with BAT received ECP, MMF, or ibrutinib; ORR at week 24 was1*†
- ECP: 29.1% (16/55; CR, 1.8%; PR, 27.3%), MMF: 28.6% (10/35; CR, 2.9%; PR, 25.7%), ibrutinib: 22.2% (6/27; CR, 7.4%; PR, 14.8%)4
*The 74% value is based on the number of patients treated with BAT (n=158). ORRs for the remaining BATs were 20% (1/5) for everolimus, 25% (2/8) for imatinib, 20% (1/5) for infliximab, 30% (3/10) for low-dose MTX, 16.7% (1/6) for rituximab, and 28.6% (2/7) for sirolimus.1,4
†REACH3 was not powered to compare ORR for Jakafi to individual BATs.
BAT=best available therapy; cGVHD=chronic graft-versus-host disease; CI=confidence interval; CR=complete response; ECP=extracorporeal photopheresis; MMF=mycophenolate mofetil; MTX=methotrexate; NIH=National Institutes of Health; OR=odds ratio; ORR=overall response rate; PR=partial response; REACH=Ruxolitinib in patiEnts with refrACtory graft-versus-Host disease after allogeneic stem cell transplantation.
Study design
REACH3 Study Design1,3

- Inclusion criteria1*
- Age 12 and older
- Allogeneic stem cell transplant from any donor source and donor type
- SR/SD cGVHD per NIH consensus criteria (moderate or severe)
- Evident myeloid and platelet engraftment
- In the Jakafi Prescribing Information, efficacy was based on ORR through week 24 (cycle 7, day 1)3
*Organ involvement at baseline for all patients (N=329): skin (71.1%), mouth (60.8%), eyes (57.4%), lungs (42.9%), joints and fascia (27.4%), liver (24.9%), GI tract (22.8%), genital tract (9.4%), missing (0.3%). Organ involvement was based on NIH consensus staging criteria at screening. A score of ≥1 was counted as organ involvement. Patients with missing assessments of single organs were counted as having no organ involvement for the organ assessed.1
aCrossover from BAT to Jakafi was permitted on or after week 24 if patients progressed, had a mixed or unchanged response, developed toxicity to BAT, or experienced a cGVHD flare. 61 patients crossed over to Jakafi after week 24. 72% of those who crossed over remained on Jakafi longer than 24 weeks.1,2
bBAT was chosen by the investigator prior to randomization: Options included ibrutinib, ECP, low-dose MTX, MMF, rituximab, everolimus, sirolimus, imatinib, infliximab, and pentostatin.3
cDefined as the proportion of patients with CR or PR at week 24.1
dDefined as the earliest time from date of randomization to relapse or recurrence of underlying disease or death due to underlying disease, nonrelapse mortality, or addition or initiation of another systemic therapy for cGVHD.1
eDefined as a ≥7-point reduction from baseline in total symptom score on the mLSS, which measures the symptoms of cGVHD on a scale of 0 to 100, with higher scores indicating worse symptoms.1
BAT=best available therapy; BID=twice daily; cGVHD=chronic graft-versus-host disease; CNI=calcineurin inhibitor; CR=complete response; ECP=extracorporeal photopheresis; FFS=failure-free survival; GI=gastrointestinal; mLSS=modified Lee Symptom Scale; MMF=mycophenolate mofetil; MTX=methotrexate; NIH=National Institutes of Health; ORR=overall response rate; PR=partial response; REACH=Ruxolitinib in patiEnts with refrACtory graft-versus-Host disease after allogeneic stem cell transplantation; SD=steroid-dependent; SR=steroid-refractory.
BAT=best available therapy; cGVHD=chronic graft-versus-host disease; CI=confidence interval; CR=complete response; FFS=failure-free survival; OR=odds ratio; ORR=overall response rate; PR=partial response; REACH=Ruxolitinib in patiEnts with refrACtory graft-versus-Host disease after allogeneic stem cell transplantation.
References: 1. Zeiser R, Polverelli N, Ram R, et al; for the REACH3 Investigators. Ruxolitinib for glucocorticoid-refractory chronic graft-versus-host disease. N Engl J Med. 2021;385(3):228-238. Supplementary appendix available at: https://www.nejm.org/doi/full/10.1056/NEJMoa2033122. 2. Data on file. Incyte Corporation. Wilmington, DE. 3. Jakafi [package insert]. Wilmington, DE: lncyte Corporation. 4. Locatelli F; for the REACH3 Study Group. Ruxolitinib vs best available therapy in patients with steroid-refractory/dependent chronic graft-vs-host disease: subgroup analyses of overall response rate in the phase 3 REACH3 trial. Presented at: 47th Annual Meeting of the EBMT; March 14-17. 2021; Rome, Italy.