
Erythema BSA involvement was associated with*:
(HR, 1.33; 95% CI, 1.19-1.48; P<0.001)2
(HR, 1.28 per 10% increase in BSA; 95% CI, 1.14-1.44; P<0.001)2

In practice, we monitor skin disease as a surrogate for disease progression—as GVHD is a systemic disease—and take an assertive approach with Jakafi treatment to help halt that progression.
Preet M. Chaudhary, MD, PhD, GVHD Expert
*In the chronic GVHD Consortium, a multicenter prospective cohort study of 469 patients with cGVHD.2

NIH Consensus Criteria3

If I don’t see at least some response within the first week or I am unable to taper steroid use, I intervene with Jakafi as opposed to taking the chance that the disease could become more severe.
Karolina Faysman, MSN, AOCNP, GVHD Expert

The potential for irreversible organ damage makes timely diagnosis critical4-7
In a prospective single-center study of 115 patients who developed cGVHD beyond day 100 after hematopoietic stem cell transplant, maximum grade was reached at a median of 6 months (range, 1-16 months) after onset of cGVHD.8
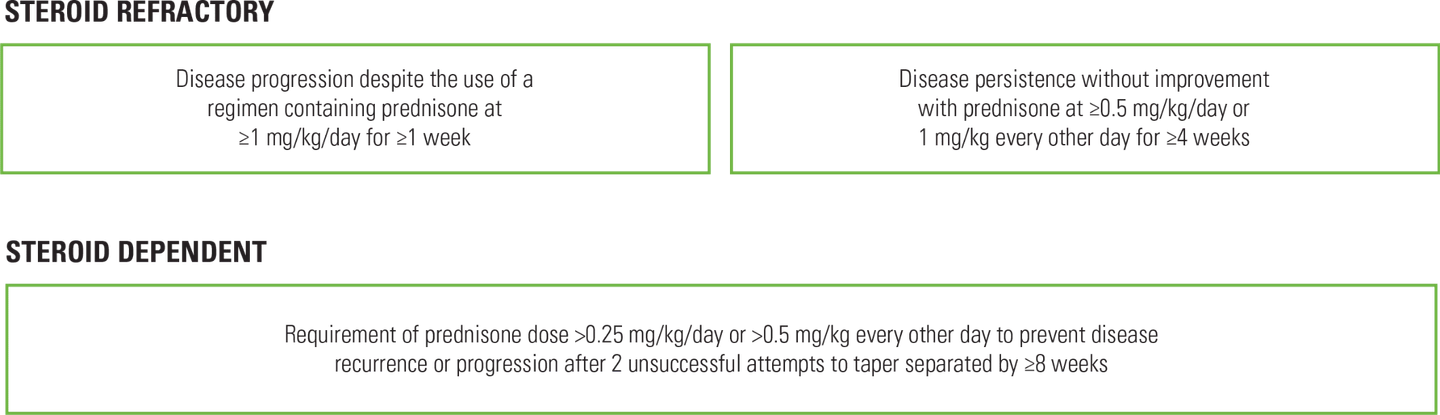
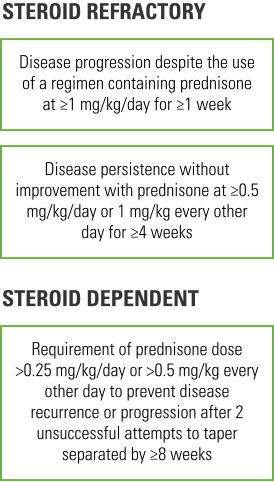
Response to daily systemic steroids3,9
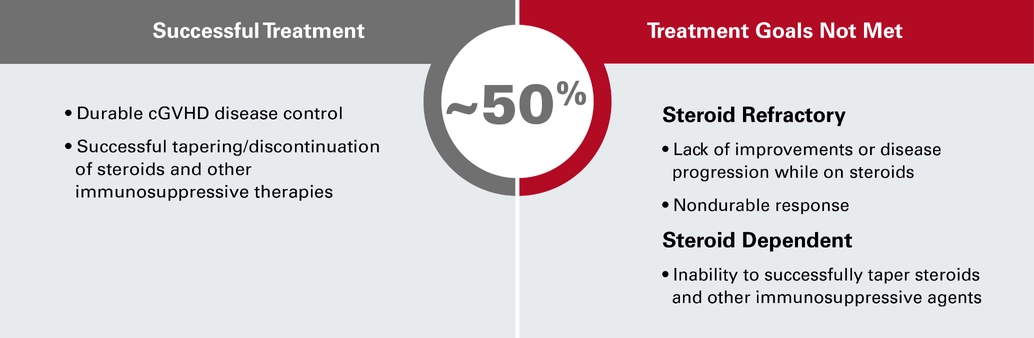
CI=confidence interval; cGVHD=chronic graft-versus-host disease; HR=hazard ratio; NIH=National Institutes of Health; SD=steroid dependent; SR=steroid refractory.
References: 1. Lueck C, Tzalavras A, Wohlfarth P, et al. Impact of chronic graft-versus-host-disease on intensive care outcome in allogeneic hematopoietic stem cell recipients. Bone Marrow Transplant. 2023;58(3):303-310. 2. Baumrin E, Baker LX, Byrne M, et al. Prognostic value of cutaneous disease severity estimates on survival outcomes in patients with chronic graft-vs-host disease. JAMA Dermatol. 2023;159(4):393-402. 3. Schoemans HM, Lee SJ, Ferrara JL, et al; for the EBMT Transplant Complications Working Party and the EBMT−NIH−CIBMTR GvHD Task Force. EBMT–NIH–CIBMTR Task Force position statement on standardized terminology & guidance for graft-versus-host disease assessment. Bone Marrow Transplant. 2018;53(11):1401-1415. 4. Lee SJ, Vogelsang G, Flowers MED. Chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2003;9(4):215-233. 5. Lee SJ, Flowers MED. Recognizing and managing chronic graft-versus-host disease. Hematology Am Soc Hematol Educ Program. 2008;228(1):134-141. 6. Nassiri N, Eslani M, Panahi N, Mehravaran S, Ziaei A, Djalilian AR. Ocular graft versus host disease following allogeneic stem cell transplantation: a review of current knowledge and recommendations. J Ophthalmic Vis Res. 2013;8(4):351-358. 7. Hildebrandt GC, Fazekas T, Lawitschka A, et al. Diagnosis and treatment of pulmonary chronic GVHD: report from the consensus conference on clinical practice in chronic GVHD. Bone Marrow Transplant. 2011;46(10):1283-1295. 8. Kuzmina Z, Eder S, Böhm A, et al. Significantly worse survival of patients with NIH-defined chronic graft-versus-host disease and thrombocytopenia or progressive onset type: results of a prospective study. Leukemia. 2012;26(4):746-756. 9. MacDonald KPA, Betts BC, Couriel D. Emerging therapeutics for the control of chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2018;24(1):19-26.