MF management should focus on achieving 3 key treatment goals, including overall survival1,2
When managing patients with MF, my goals include control of the
SPLEEN and SYMPTOMS, with an ultimate goal of OVERALL
SURVIVAL.
When managing patients with MF, my goals include control of the SPLEEN and SYMPTOMS, with an ultimate goal of OVERALL SURVIVAL.
Ruben Mesa, MD, FACP, MPN Expert
Palpable spleen is a marker of disease progression and is associated with poor OS3,4
- A palpable spleen of ≥5 cm below the left costal margin constitutes progressive disease,† according to the IWG-MRT and ELN response criteria3
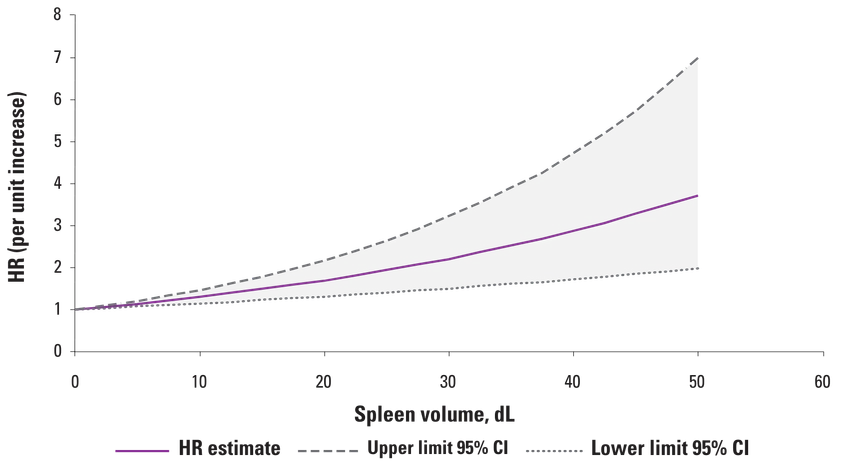
Larger baseline spleen volume was associated with incremental increases in the risk of death4
This material is under a CC BY-NC License and is the property of the Ferrata Storti Foundation. © 2023 Ferrata Storti Foundation. All rights reserved.
- In a post hoc pooled analysis of OS in the COMFORT studies (N=528), there was a 14% increase in the risk of death for each additional 5 dL in spleen volume at baseline over 3 years (HR, 1.14; 95% CI, 1.07-1.21)4‡
- These increases were seen irrespective of treatment5
When my adult patients with intermediate- to high-risk myelofibrosis are experiencing any degree of splenomegaly at diagnosis, that is a sign that I need to intervene with Jakafi.
- *Data were available for 768 patients, 681 of whom had palpable splenomegaly.5
- †Progressive disease assignment for splenomegaly requires confirmation by CT or MRI showing a ≥25% increase in spleen volume from baseline. Baseline values for both physical examination and imaging studies refer to pretreatment baseline and not to posttreatment measurements.3
- ‡A post hoc pooled analysis of OS with ruxolitinib was performed using data from 2 phase 3 studies: COMFORT-I, a randomized, double-blind, placebo-controlled study with 309 patients with intermediate-2-risk or high-risk MF, and COMFORT-II, a randomized, open-label study with 219 patients with intermediate-2-risk or high-risk MF. The primary endpoint in both studies was the proportion of patients achieving a ≥35% reduction in spleen volume (measured by CT or MRI)—at week 24 in COMFORT-I and at week 48 in COMFORT-II.4,6,7
CI=confidence interval; COMFORT=COntrolled MyeloFibrosis study with ORal JAK inhibitor Treatment; CT=computed tomography; ELN=European LeukemiaNet; HR=hazard ratio; IWG-MRT=International Working Group-Myeloproliferative Neoplasms Research and Treatment; MF=myelofibrosis; MPN=myeloproliferative neoplasm; MRI=magnetic resonance imaging; OS=overall survival; SVR=spleen volume reduction.
References: 1. Barbui T, Barosi G, Birgegard G, et al. Philadelphia-negative classical myeloproliferative neoplasms: critical concepts and management recommendations from European LeukemiaNet. J Clin Oncol. 2011;29(6):761-770. 2. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Myeloproliferative Neoplasms V.2.2023. © National Comprehensive Cancer Network, Inc. 2023. All rights reserved. Accessed June 23, 2023. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way. 3. Tefferi A, Cervantes F, Mesa R, et al. Revised response criteria for myelofibrosis: International Working Group-Myeloproliferative Neoplasms Research and Treatment (IWG-MRT) and European LeukemiaNet (ELN) consensus report. Blood. 2013;122(8):1395-1398. 4. Vannucchi AM, Kantarjian HM, Kiladjian J-J, et al; on behalf of the COMFORT Investigators. A pooled analysis of overall survival in COMFORT-I and COMFORT-II, 2 randomized phase III trials of ruxolitinib for the treatment of myelofibrosis. Haematologica. 2015;100(9):1139-1145. 5. Cervantes F, Dupriez B, Pereira A, et al. New prognostic scoring system for primary myelofibrosis based on a study of the International Working Group for Myelofibrosis Research and Treatment. Blood. 2009;113(13):2895-2901. 6. Harrison CN, Vannucchi AM, Kiladjian J-J, et al; on behalf of the COMFORT-II Investigators. Long-term findings from COMFORT-II, a phase 3 study of ruxolitinib vs best available therapy for myelofibrosis. Leukemia. 2016;30(8):1701-1707. 7. Verstovsek S, Mesa RA, Gotlib J, et al. A double-blind, placebo-controlled trial of ruxolitinib for myelofibrosis. N Engl J Med. 2012;366(9):799-807. Supplementary appendix available at: https://www.nejm.org/doi/full/10.1056/nejmoa1110557.