For adults with intermediate- or high-risk MF1
At diagnosis, intervene with Jakafi® (ruxolitinib): A treatment with 5-year overall survival data1-4
COMFORT-I primary endpoint*
of patients receiving Jakafi achieved a ≥35% reduction in spleen volume at week 24 vs 0.7% of patients receiving placebo (P<0.0001)1,5
- 4.4 years median duration of spleen response among primary responders (n=65)2†
- 99% of patients experienced some reduction in spleen volume on Jakafi5,6
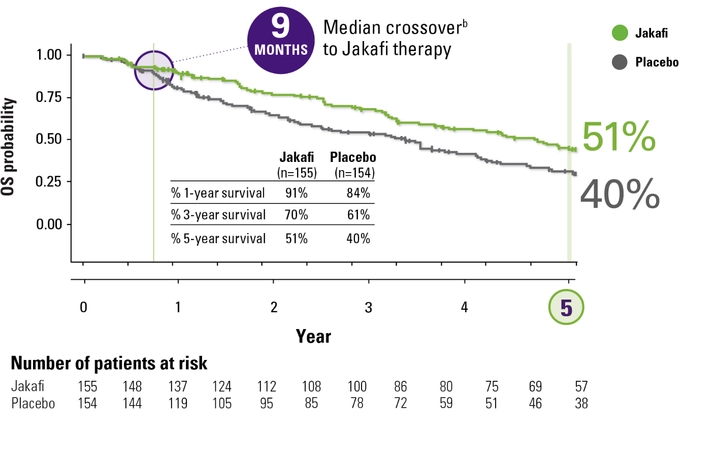
COMFORT-I 5-year OS analysis‡: Jakafi and placebo
- At 3 years, survival probability was 70% for patients originally randomized to Jakafi and 61% for those originally randomized to placebo1
- OS was a prespecified secondary endpoint in COMFORT-I1
OS Kaplan-Meier Curves by Treatment Group in COMFORT-I1-3,a


As a clinician, I want a therapy that can meet my treatment goals. And seeing the impact of Jakafi on spleen volume reduction and overall survival gives me the confidence to intervene with Jakafi at diagnosis, instead of watching and waiting.
HEAR MORE ABOUT SVR AND OS FROM DR MESA
COMFORT-II primary endpoint§
of patients receiving Jakafi achieved a ≥35% reduction in spleen volume at week 48 vs 0% of patients receiving BAT‖ (P<0.0001)1,7
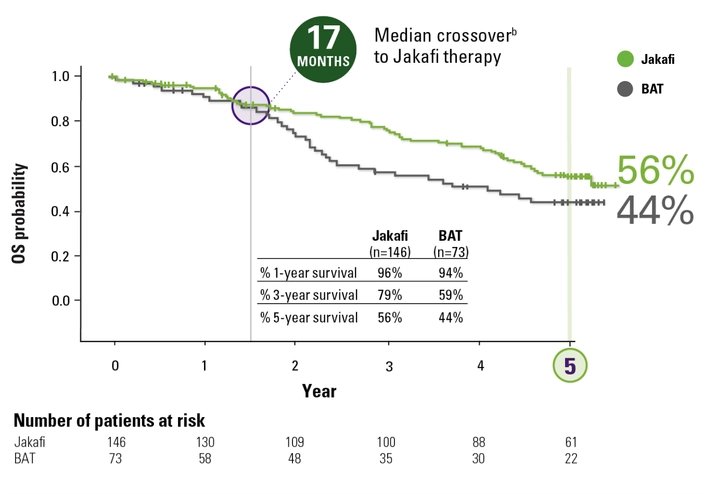
COMFORT-II 5-year OS analysis‡: Jakafi and BAT
- At 3 years, survival probability was 79% for patients originally randomized to Jakafi and 59% for those originally randomized to BAT1
- OS was a prespecified secondary endpoint in COMFORT-II1
OS Kaplan-Meier Curves by Treatment Group in COMFORT-II1,4,a

I do not use hydroxyurea for my myelofibrosis patients. The overall survival data available from COMFORT studies give me the confidence of prescribing Jakafi for my appropriate patients at diagnosis and not to delay the treatment.
HEAR HOW DR FAZAL APPROACHES ACTIVE MANAGEMENT
References: 1. Jakafi [package insert]. Wilmington, DE: Incyte Corporation. 2. Data on file. Incyte Corporation. Wilmington, DE. 3. Verstovsek S, Mesa RA, Gotlib J, et al; for the COMFORT-I investigators. Long-term treatment with ruxolitinib for patients with myelofibrosis: 5-year update from the randomized, double-blind, placebo-controlled, phase 3 COMFORT-I trial. J Hematol Oncol. 2017;10(1):55. 4. Harrison CN, Vannucchi AM, Kiladjian J-J, et al; on behalf of the COMFORT-II Investigators. Long-term findings from COMFORT-II, a phase 3 study of ruxolitinib vs best available therapy for myelofibrosis. Leukemia. 2016;30(8):1701-1707. 5. Verstovsek S, Mesa RA, Gotlib J, et al. A double-blind, placebo-controlled trial of ruxolitinib for myelofibrosis. N Engl J Med. 2012;366(9):799-807. Supplementary appendix available at: https://www.nejm.org/doi/full/10.1056/nejmoa1110557. 6. Deisseroth A, Kaminskas E, Grillo J, et al. US Food and Drug Administration approval: ruxolitinib for the treatment of patients with intermediate and high-risk myelofibrosis. Clin Cancer Res. 2012;18(12):3212-3217. 7. Harrison C, Kiladjian J-J, Al-Ali HK, et al. JAK inhibition with ruxolitinib versus best available therapy for myelofibrosis. N Engl J Med. 2012;366(9):787-798.