For adults with intermediate- or high-risk MF1
Intervene with Jakafi® (ruxolitinib) at diagnosis, regardless of anemia
In my practice, there is no hemoglobin level that precludes me from starting my appropriate patients with MF on Jakafi.
Ruben Mesa, MD, FACP, MPN Expert
COMFORT-I*
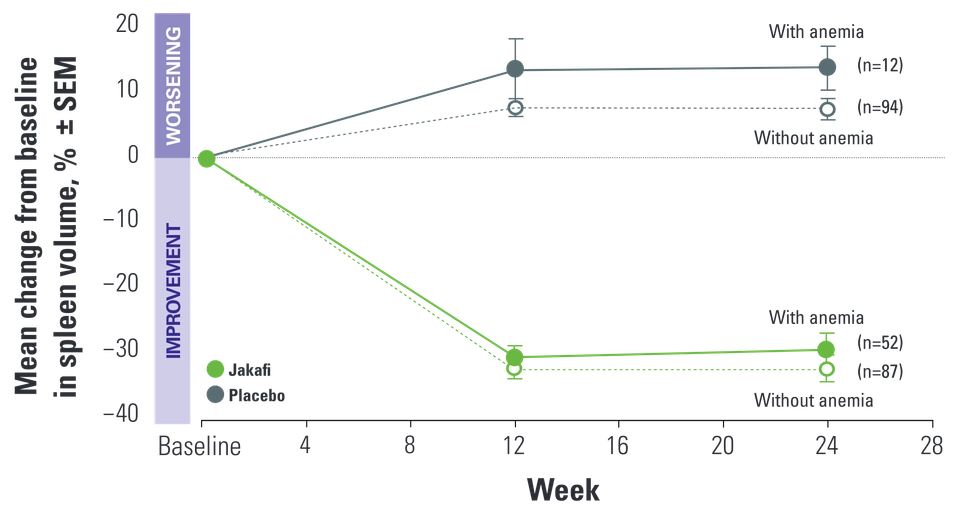
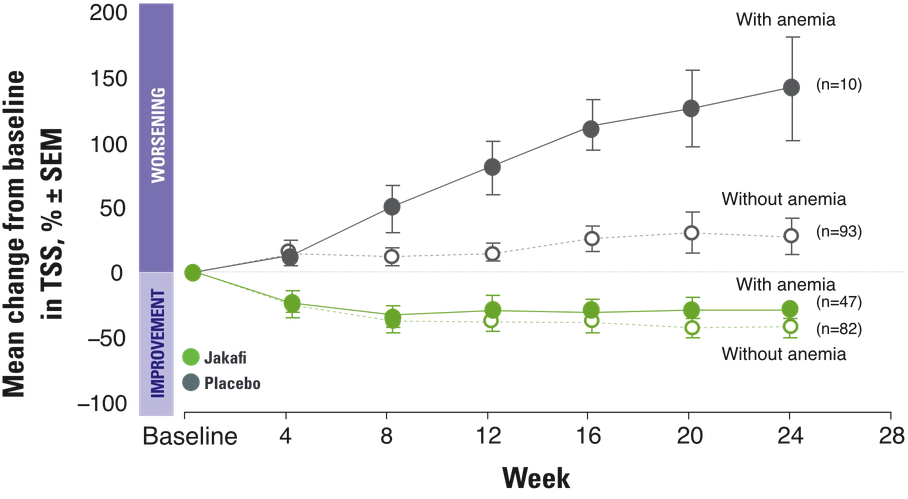
Jakafi significantly reduced spleen volume and improved symptoms. Results were consistent in patients with new-onset anemia1,2
There are no contraindications for the use of Jakafi, including in patients with anemia1
- In COMFORT-I, 46% of patients receiving Jakafi had anemia at baseline†; among these patients, mean Hb was 9.2 g/dL (range, 6.6 g/dL to 13.7 g/dL)3
COMFORT-I additional analysis: New-onset anemia did not impact efficacy for patients on Jakafi2,3
COMFORT-I rates of anemia1,2

<1% of patients receiving Jakafi in the COMFORT-I study discontinued due to anemia2
Identification and management of new-onset anemia
- Perform a pretreatment CBC, and monitor CBCs every 2 to 4 weeks until doses are stabilized, and then as clinically indicated1
- Dose modifications and/or blood transfusions may be required for patients who develop anemia1
Hb partially recovered to a new steady state after initial decrease and remained stable over time4
COMFORT-I: Mean Hb Levels Over Time4
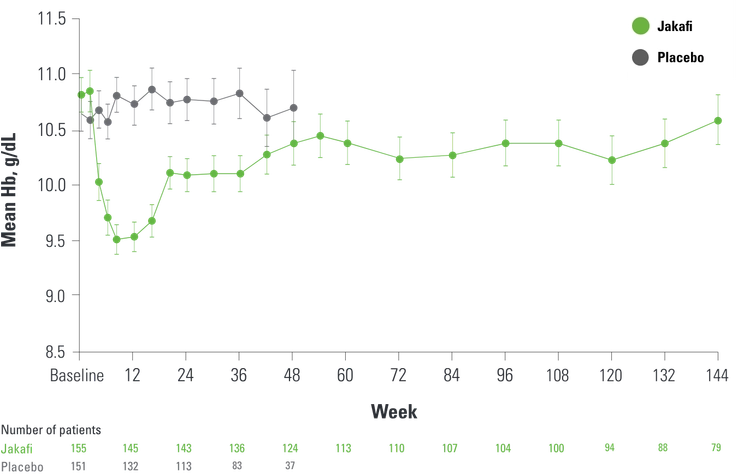
- Mean decreases in Hb levels reached a nadir of approximately 1.5 g/dL to 2 g/dL below baseline after 8 to 12 weeks of therapy and then gradually recovered to reach a new steady state that was approximately 1 g/dL below baseline4


When I do have a patient with anemia, I first educate them that a decrease in hemoglobin is to be expected, typically within the range of 1.5 and 2 grams per deciliter. This decrease is typically front-loaded; however, it is often transient. I also explain that a decrease in hemoglobin levels may not limit the impact or long-term outcomes of Jakafi.
HEAR MORE ABOUT HOW DR MESA MANAGES ANEMIA
By week 36, the proportion of patients on Jakafi requiring RBC transfusions‡ decreased to levels similar to placebo and remained stable over time5
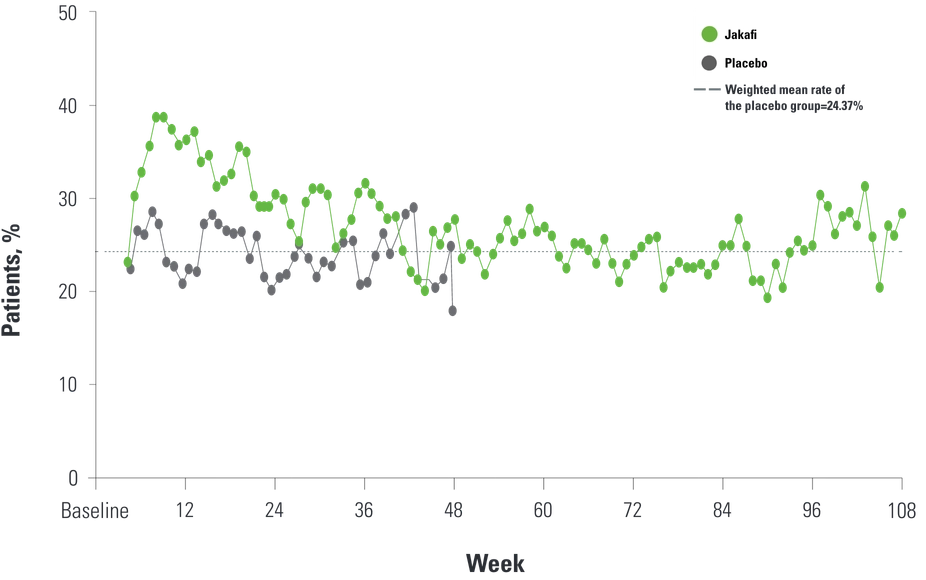
- Through week 24, 60% of patients treated with Jakafi and 38% of patients receiving placebo required RBC transfusions1
- 123 of 155 patients receiving Jakafi were transfusion independent at baseline, compared with 119 of 151 receiving placebo. Of the 123 transfusion-independent patients receiving Jakafi, 27% became transfusion dependent§ during the 8 weeks before data cutoff, compared with 14% receiving placebo3
- During randomized treatment, 41% of patients treated with Jakafi and 47% of patients treated with placebo became newly transfusion independent2
The COMFORT-I study gives me the confidence to not only initiate Jakafi at diagnosis for my patients with MF who have anemia at baseline, but also manage through that anemia while on treatment. And we see in the data that the benefits of Jakafi may balance the potential concerns for anemia.
Ruben Mesa, MD, FACP, MPN Expert

*COMFORT-I was a randomized, double-blind, placebo-controlled, phase 3 study with 309 patients with intermediate-2–risk or high-risk MF. The primary endpoint was the proportion of patients achieving a ≥35% reduction in spleen volume from baseline to week 24 as measured by CT or MRI.1,3
†Anemia at baseline was defined as RBC transfusion within the first 12 weeks prior to the initial dose of Jakafi, or baseline Hb <10 g/dL.2
‡One or more units of RBCs.5
§New-onset transfusion dependency: the use of 2 or more units of RBC product(s) during the final 8 weeks before data-cutoff date in a patient who was not transfusion dependent at baseline.2
BAT=best available therapy; CBC=complete blood count; COMFORT=COntrolled MyeloFibrosis study with ORal JAK inhibitor Treatment; CT=computed tomography; Hb=hemoglobin; JUMP=JAK Inhibitor RUxolitinib in Myelofibrosis Patients; MF=myelofibrosis; MPN=myeloproliferative neoplasm; MRI=magnetic resonance imaging; OS=overall survival; RBC=red blood cell; SEM=standard error of the mean; TSS=Total Symptom Score.
References: 1. Jakafi [package insert]. Wilmington, DE: Incyte Corporation. 2. Verstovsek S, Mesa RA, Gotlib J, et al. A double-blind, placebo-controlled trial of ruxolitinib for myelofibrosis. N Engl J Med. 2012;366(9):799-807. Supplementary appendix available at: https://www.nejm.org/doi/full/10.1056/nejmoa1110557. 3. Data on file. Incyte Corporation. Wilmington, DE. 4. Verstovsek S, Mesa RA, Gotlib J, et al. Efficacy, safety, and survival with ruxolitinib in patients with myelofibrosis: results of a median 3-year follow-up of COMFORT-I. Haematologica. 2015;100(4):479-488. 5. Verstovsek S, Mesa RA, Gotlib J, et al. Efficacy, safety and survival with ruxolitinib in patients with myelofibrosis: results of a median 2-year follow-up of COMFORT-I. Haematologica. 2013;98(12):1865-1871. Supplementary appendix available at: https://haematologica.org/article/view/6861.