Significantly more patients on Jakafi® (ruxolitinib) achieved a complete response vs BAT1
In the phase 3 RESPONSE* trial, Jakafi demonstrated superior results† vs BAT2‡
RESPONSE composite primary endpoint2
(25/110) of patients receiving Jakafi achieved Hct control and ≥35% spleen volume reduction at week 32 vs <1% (1/112) of patients receiving BAT (P<0.0001)§
MAJIC-PV study design1
- MAJIC-PV was an open-label, phase 2, randomized, controlled trial of Jakafi vs BAT|| conducted in patients with high-risk PV meeting criteria for being resistant/intolerant to HU (N=180)
- There was no per-protocol crossover of BAT patients to Jakafi¶
- Primary endpoint was complete response (CR) rate within 12 months as defined by ELN criteria: Hct <45% without phlebotomy for 3 months, platelets ≤400 × 109/L, WBC count ≤10 × 109/L, and normal spleen size
- Apart from the primary endpoint, all additional endpoints were exploratory and unpowered
MAJIC-PV primary endpoint: Significantly more patients on Jakafi achieved a CR vs BAT1
MAJIC-PV secondary endpoint
Jakafi EFS and thrombosis-free survival vs BAT1
- Jakafi demonstrated a 42% reduction in the risk of an event vs BAT (HR, 0.58; 95% CI, 0.35-0.94)
- EFS was a composite of major thrombosis, major hemorrhage, transformation, or death
Kaplan-Meier Analysis: Thrombosis-Free Survival1
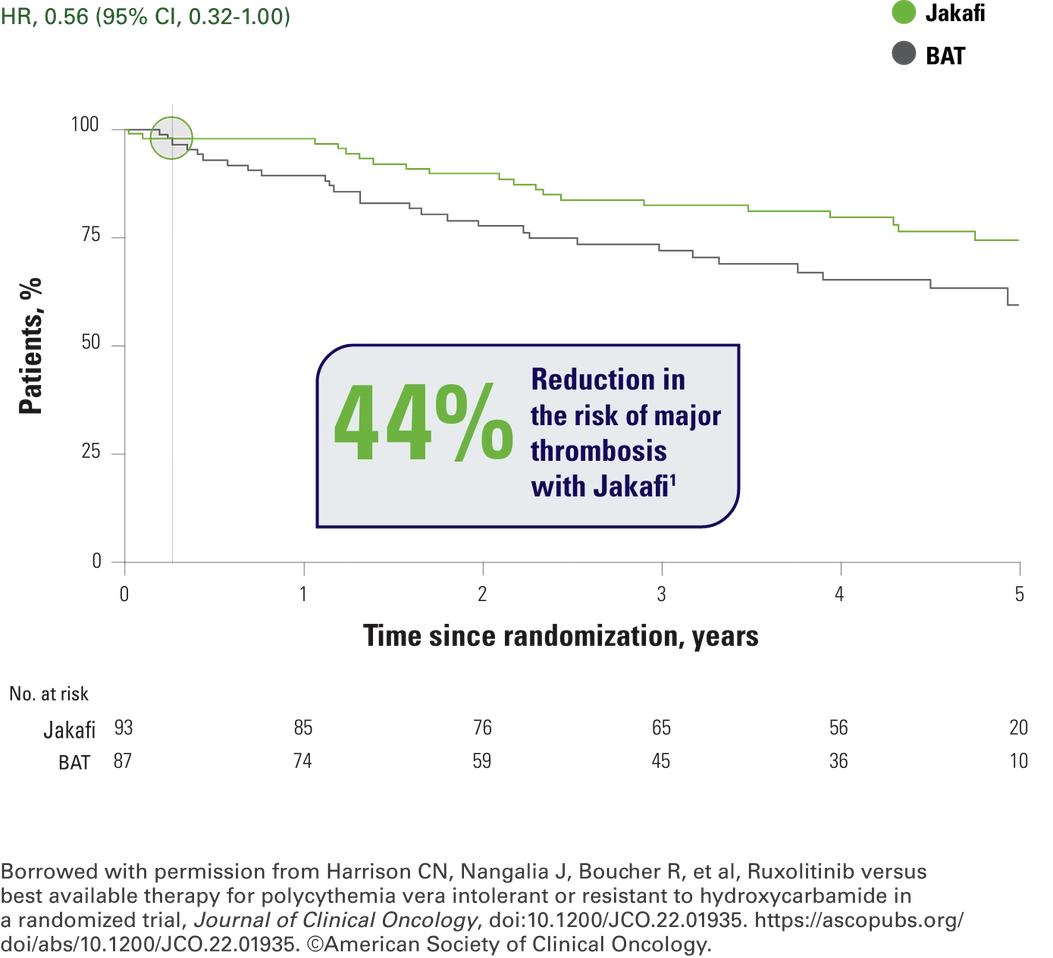


As you can see, the separation between the curves happens early on and they remain separated throughout the study. It’s important to remember that inclusion criteria for the study was hydroxyurea resistance. So, from my perspective, these data also tell me that we need to sit up and take notice immediately, because my patients showing signs of hydroxyurea resistance may be at increased risk of major thrombosis.

Jakafi safety data: MAJIC-PV trial1
MAJIC-PV AEs1
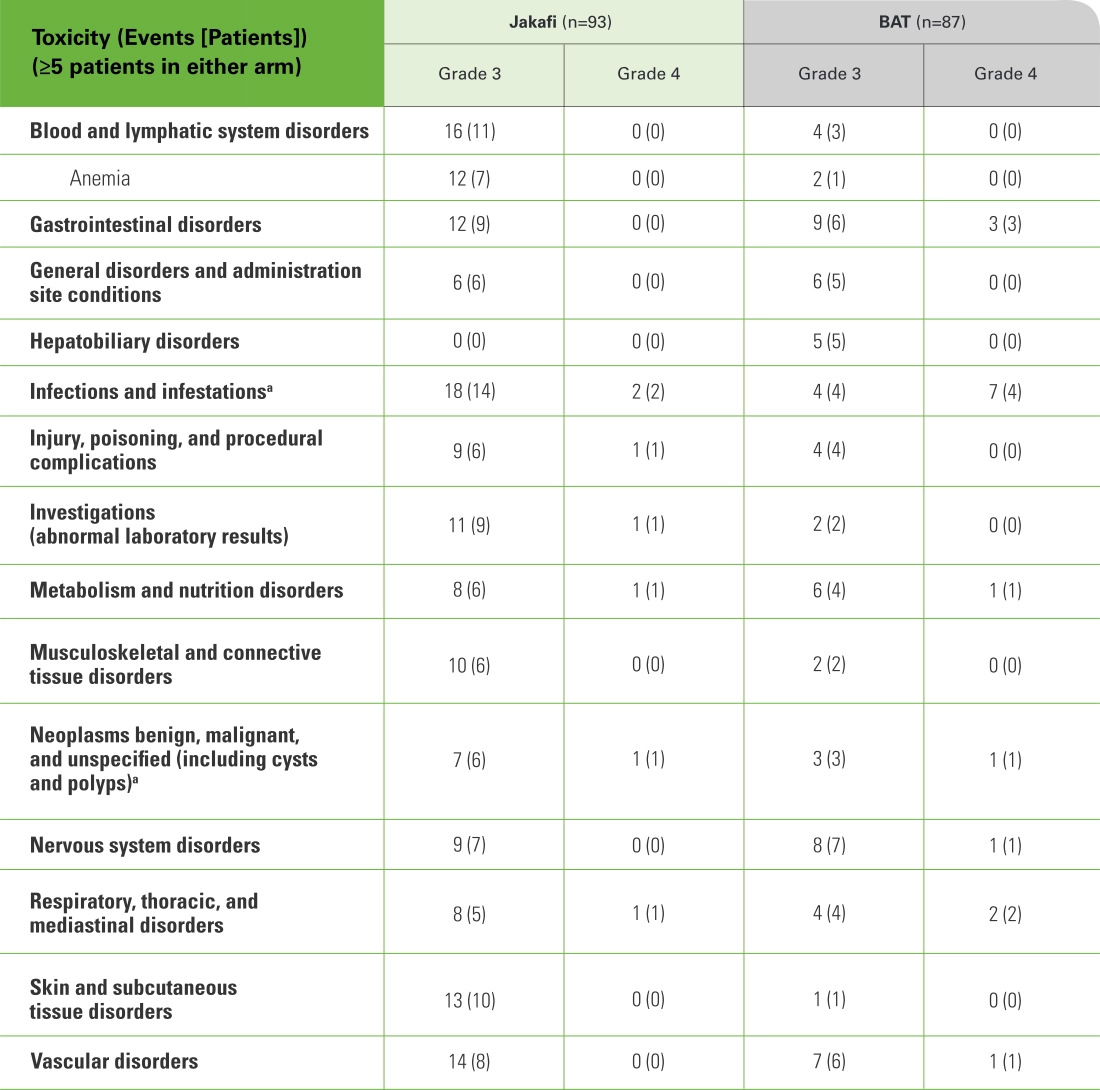
- aMalignancies and infections were deemed AEs of special interest and have been presented separately. See MAJIC supplementary information.
- No grade 5 events occurred in the Jakafi arm, and 3 grade 5 events (1 intracranial hemorrhage and 2 vascular disorders) occurred in the BAT arm1
- Squamous cell skin cancer was reported more commonly with Jakafi compared with BAT (11 vs 0 events, respectively)1
- *The RESPONSE trial was a randomized, open-label, active-controlled phase 3 trial comparing Jakafi with BAT in 222 patients with PV. Patients enrolled in the study had been diagnosed with PV for at least 24 weeks, had an inadequate response to or were intolerant of HU, required phlebotomy for Hct control, and exhibited splenomegaly. All patients were required to demonstrate Hct control between 40% and 45% prior to randomization. After week 32, patients on BAT were able to cross over to Jakafi treatment.2,3
- †The composite primary endpoint was defined as Hct control without phlebotomy eligibility and a ≥35% spleen volume reduction as measured by CT or MRI. To achieve the Hct control endpoint, patients could not become eligible for phlebotomy between weeks 8 and 32. Phlebotomy eligibility was defined as Hct >45% that is ≥3 percentage points higher than baseline or Hct >48% (lower value).2,3
- ‡BAT included HU (60%), interferon/pegylated interferon (12%), anagrelide (7%), pipobroman (2%), lenalidomide/thalidomide (5%), and observation (15%).2
- §Jakafi: 95% CI, 0.15-0.32; BAT: 95% CI, 0.00-0.05.2
- ∥BAT included HU (32%), interferon (15%), HU/interferon (11%), anagrelide/HU (10%), anagrelide (3%), anagrelide/interferon (3%), anagrelide/HU/interferon (3%), busulfan/interferon (2%), interferon/ruxolitinib (2%), HU/interferon/ruxolitinib (3%), anagrelide/ruxolitinib (1%), anagrelide/interferon/ruxolitinib (1%), anagrelide/ HU/interferon/ruxolitinib (1%), busulfan/HU/interferon (1%), busulfan/ruxolitinib (1%), HU/ruxolitinib (1%), interferon/pipobroman (1%), 32P (1%), busulfan (1%), 32P/HU (1%), 32P/anagrelide/interferon (1%).1
- ¶Patients receiving BAT were permitted to change therapy; 66% (57 of 87) continued with HU as BAT. Ten patients received Jakafi treatment in the BAT arm.1
32P=radiophosphorus 32; AE=adverse event; BAT=best available therapy; CI=confidence interval; CT=computed tomography; EFS=event-free survival; ELN=European LeukemiaNet; Hct=hematocrit; HR=hazard ratio; HU=hydroxyurea; MPN=myeloproliferative neoplasm; MRI=magnetic resonance imaging; PV=polycythemia vera; RESPONSE=Randomized study of Efficacy and Safety in POlycythemia vera with JAK iNhibitor ruxolitinib verSus bEst available care; WBC=white blood cell.
References: 1. Harrison CN, Nangalia J, Boucher R, et al. Ruxolitinib versus best available therapy for polycythemia vera intolerant or resistant to hydroxycarbamide in a randomized trial. J Clin Oncol. 2023;41(19):3534-3544. Supplemental information available at: https://ascopubs.org/doi/suppl/10.1200/JCO.22.01935. 2. Jakafi [package insert]. Wilmington, DE: Incyte Corporation. 3. Vannucchi AM, Kiladjian JJ, Griesshammer M, et al. Ruxolitinib versus standard therapy for the treatment of polycythemia vera. N Engl J Med. 2015;372(5):426-435. Supplementary appendix available at: https://www.nejm.org/doi/suppl/10.1056/NEJMoa1409002/suppl_file/nejmoa1409002_appendix.pdf.