For PV in adults who have had an inadequate response to or are intolerant of HU1
Once-daily dosing with JAKAFI XR™ (ruxolitinib)1
Dose optimization is key to maintaining the balance between safety and efficacy1
- For patients with PV who have an inadequate response to or are intolerant of HU, the recommended starting dose of JAKAFI XR is 22 mg once daily
- A CBC must be performed before initiating JAKAFI XR
- Before initiating JAKAFI XR, inquire about past infections, including tuberculosis, herpes simplex, herpes zoster, and hepatitis B
- JAKAFI XR is dosed orally and can be administered with or without food
- Patients must swallow JAKAFI XR tablets whole. Do not split, chew, or crush tablets

JAKAFI® (ruxolitinib) and JAKAFI XR doses:
JAKAFI dosages
5 mg twice daily
Image
10 mg twice daily
Image
15 mg twice daily
Image
20 mg twice daily
Image
25 mg twice daily
Image
JAKAFI XR dosages
11 mg once daily
Image
22 mg once daily
Image
33 mg once daily
Image
44 mg once daily
Image
55 mg once daily
Image
-
Image
-
Image

-
Image
-
Image

Tablet images shown are for demonstration purposes only and do not represent actual medications.
Dose modifications should be considered based on monitoring complete blood count (CBC), including platelet counts, absolute neutrophil count (ANC), and hemoglobin; treatment interruption and restarting dosing; or other adverse reactions, as described in the Full Prescribing Information for JAKAFI and JAKAFI XR.
During treatment with JAKAFI XR
- A CBC must be performed before initiating JAKAFI XR, every 2 to 4 weeks until doses are stabilized, and then as clinically indicated
- Assess lipid parameters approximately 8 to 12 weeks following initiation of JAKAFI XR
Missed dose
- If a dose is missed, patients should not take an additional dose but should take the next usual prescribed dose
Individualize dosing of JAKAFI XR to optimize the balance between safety and efficacy
- Dosing may be reduced or temporarily interrupted based on hemoglobin, platelet, or neutrophil counts
- Additionally, dosing may be increased to achieve desired clinical response
- Interrupt treatment for bleeding
HU=hydroxyurea; PV=polycythemia vera.
The effectiveness and safety of JAKAFI XR have been established based on adequate and well-controlled studies of JAKAFI
JAKAFI XR received approval based on comprehensive data demonstrating bioequivalence to JAKAFI1
Decrease dose for anemia or thrombocytopenia1

Hb=hemoglobin.
Increase dose for insufficient response1
If the response is insufficient and platelet, Hb, and neutrophil counts are adequate, JAKAFI XR doses may be increased in increments of 11 mg once daily to a maximum of 55 mg once daily
- Doses should not be increased during the first 4 weeks of therapy and should not be increased more frequently than every 2 weeks
Consider dose increases in patients who meet all of these criteria:
- Inadequate efficacy as demonstrated by 1 or more of the following:
- - Continued need for phlebotomy
- - WBC count greater than the ULN range
- - Platelet count greater than the ULN range
- - Palpable spleen that is reduced <25% from baseline
- Platelet count ≥140 × 109/L
- Hb ≥12 g/dL
- ANC ≥1.5 × 109/L
ANC=absolute neutrophil count; Hb=hemoglobin; ULN=upper limit of normal; WBC=white blood cell.
Interrupting/restarting dosing1
Interrupt JAKAFI XR treatment for:
- Anemia (Hb <8 g/dL),
- Thrombocytopenia (platelet count <50 × 109/L), or
- Neutropenia (ANC <1.0 × 109/L)
After recovery of hematologic parameter(s) to acceptable levels, dosing may be restarted.
Use the most severe category of patients’ Hb, platelet count, or ANC abnormality to determine the corresponding maximum restarting dose:
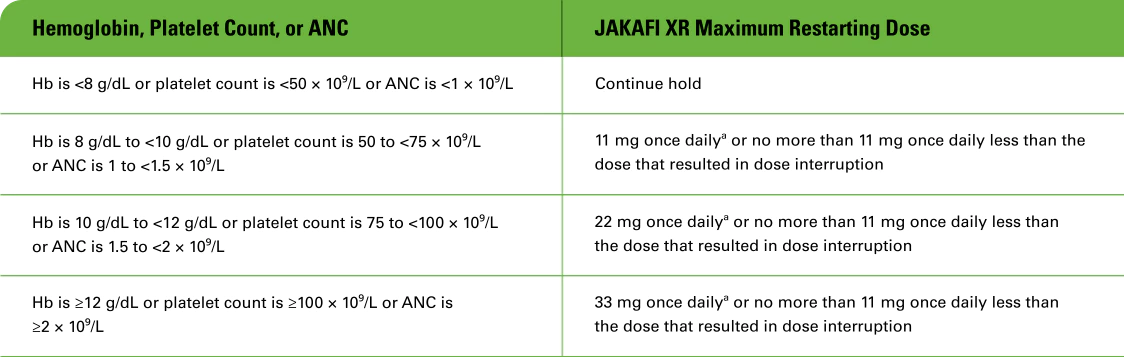
- aContinue JAKAFI XR treatment for at least 2 weeks; if stable, may increase dose by 11 mg once daily.
Patients who required dose interruption while receiving a dose of JAKAFI XR 11 mg once daily may restart JAKAFI XR at a dose of 11 mg once daily, but not higher, when they have:
- Hb ≥10 g/dL
- Platelet count ≥75 × 109/L
- ANC ≥1.5 × 109/L
Dose management after restarting treatment in PV:
- After restarting JAKAFI XR following treatment interruption, doses may be titrated, but the maximum total daily dose should not exceed 11 mg once daily less than the dose that resulted in the dose interruption
- An exception to this is dose interruption following phlebotomy-associated anemia, in which case the maximal total daily dose allowed after restarting JAKAFI XR would not be limited
Special populations:
- Avoid fluconazole doses >200 mg daily with JAKAFI XR
- Avoid use of JAKAFI XR in patients with end-stage renal disease (CLcr <15 mL/min) not requiring dialysis
ANC=absolute neutrophil count; CLcr=creatinine clearance; Hb=hemoglobin; PV=polycythemia vera.
Dose modifications for special populations1
Modify the dose of JAKAFI XR accordingly in patients with moderate or severe renal impairment, patients with hepatic impairment, and patients on dialysis.

Patients with ESRD on dialysis
- Do not use JAKAFI XR for patients with PV who have ESRD (CLcr <15 mL/min) and are on dialysis with any platelet count
- Avoid use of JAKAFI XR in patients with ESRD (CLcr <15 mL/min) not requiring dialysis
Concomitant use with strong CYP3A4 inhibitors or fluconazole
- Modify the dose of JAKAFI XR when coadministered with strong CYP3A4 inhibitors and fluconazole doses of ≤200 mg
- Avoid the use of fluconazole doses >200 mg daily with JAKAFI XR
- Additional dose modifications should be made with frequent monitoring of safety and efficacy

CLcr=creatinine clearance; ESRD=end-stage renal disease; PV=polycythemia vera.
HU=hydroxyurea; MPN=myeloproliferative neoplasm; PV=polycythemia vera.
Reference: 1. JAKAFI/JAKAFI XR Prescribing Information. Wilmington, DE: Incyte Corporation.