Perspectives and insights from PV experts
The resources on this page offer information and insights about Jakafi® (ruxolitinib) and treatment of patients with PV who have had an inadequate response to or are intolerant of HU. Be sure to check back regularly as new materials will be added as they become available.
Hct Control and WBC Reduction in Patients With PV
Hematologist-oncologist Dr Andrew Kuykendall shares how he manages progressive WBC counts and when it may be time to intervene with Jakafi.
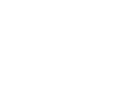
Hi, my name is Andrew Kuykendall and I'm a malignant hematologist. Today, we're going to talk about patients with polycythemia vera and the importance of strict hematocrit control as well as the value in controlling white blood cell counts in these patients.
So, we know the gold standard for treating patients with polycythemia vera is to maintain a hematocrit less than 45% due to the risk factors associated with a hematocrit value greater than 45%. Oftentimes in order to do this, we're having to intervene when hematocrit values are slightly lower than 45%, say 43 to 44%. And we need to establish a zone that we consider to be safe for these patients, maybe between 40 and 45%.
If a patient’s current dose for hydroxyurea is not adequately managing their hematocrit levels, I will try to titrate up to their maximum tolerated dose. Phlebotomy is another tool for maintaining hematocrit levels below 45% but when I get to three to six phlebotomies a year, that’s a red flag for me. It tells me the hydroxyurea is insufficient for that patient. I also find that if done too frequently the procedure can be inconvenient for patients and may put them at some risk for iron deficiency.
There are certain things that may alert us to the fact that the disease has changed, and we may need to alter our treatment plan. Beyond frequent need for phlebotomies or increasing doses of hydroxyurea, one other thing is a progressive increase in white blood cell count. If the white blood cell count is increasing from 11 to 13 to 15,000, this may indicate that we don't have good control of the leukocytosis and a change in treatment plan may be required.
It's important in patients with polycythemia vera to establish what their baseline white blood cell count is. Ideally, we want this number to be at or below 11,000 because we understand there's some risk associated with a higher baseline white blood cell count.
Patients frequently come in and ask me about their different lab values. And when they see a white blood cell count that's rising progressively, it makes them think the disease is changing. It makes them think their disease is progressive. And they wonder what we're going to do to try to get that under control.
So if I have a patient who is encountering challenges strictly maintaining hematocrit levels below 45% and has progressive leukocytosis, this tells me that hydroxyurea is no longer sufficient. This is the time I talk to patients about a change from hydroxyurea to Jakafi and findings from the response trial help support my decision.
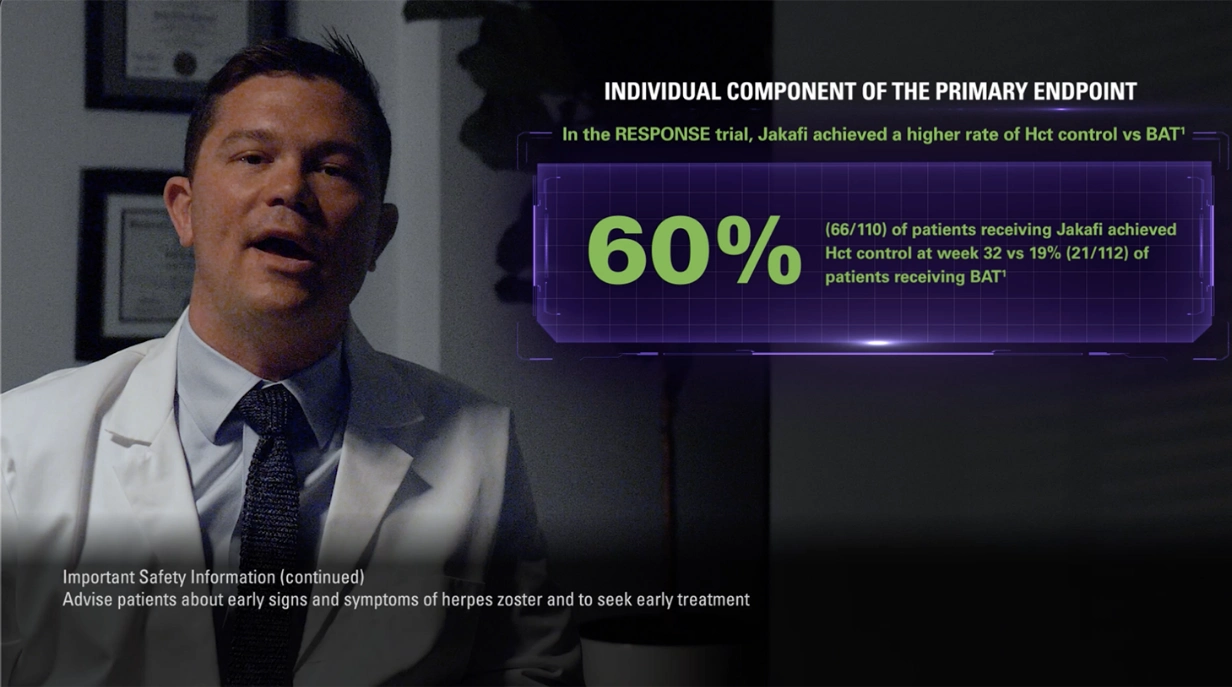
Now the RESPONSE trial was a phase three study that enrolled patients with polycythemia vera who were resistant to or intolerant of hydroxyurea and they required phlebotomy to control their hematocrit levels.
The study was designed to look at hematocrit control and reduction in spleen volume of at least 35%. Patients could not become eligible for phlebotomy between weeks 8 and 32 of the trial. And what was found in the RESPONSE trial was that significantly more patients treated with Jakafi were able to achieve that primary composite endpoint, compared to patients treated with best available therapy.
But more so than just achieving a response, long-term data matters as well because we need to know more about the durability of these responses. And patients on Jakafi actually had a 74% probability of maintaining this primary response at five years.
Now progressive leukocytosis can also indicate the need to intervene, and this is important because this was looked at on the RESPONSE trial as well, which included complete hematologic response as an endpoint.
Complete hematologic remission is an important endpoint because this includes more things. This is not just controlling the hematocrit, but it also includes controlling the platelet count and the white blood cell count. And what they found was that patients on Jakafi achieved significantly higher rates of CHR compared with patients receiving best available therapy at week 32.
And that response was durable: Patients in CHR on Jakafi had a 55% probability of remaining in remission at 5 years. Looking specifically at white blood cells, investigators looked at trends in mean white blood cell counts over time and mean change from baseline in white blood cell counts. This was an exploratory analysis done by analyzing subgroups based on therapy.
We talked earlier about using hydroxyurea to reduce white blood cell counts, and the study tracked changes from baseline for Jakafi and for hydroxyurea both in the BAT arm and on its own. The idea that we have a medication such as Jakafi that can provide control of not just hematocrit, but also of white blood cell counts can be very important and reassuring for patients.
So, in my practice, I think it's important to identify patients who are appropriate for Jakafi. These may be patients that are at maximum tolerated doses of hydroxyurea, struggling to maintain hematocrit less than or equal to 45%, and/or having progressive leukocytosis. In that setting, I think it's important to put our best foot forward and get started with Jakafi.
Let’s take the opportunity to review the safety information for Jakafi.
INDICATIONS AND USAGE
Jakafi® (ruxolitinib) is indicated for treatment of polycythemia vera (PV) in adults who have had an inadequate response to or are intolerant of hydroxyurea.
IMPORTANT SAFETY INFORMATION
- Treatment with Jakafi® (ruxolitinib) can cause thrombocytopenia, anemia and neutropenia, which are each dose-related effects. Perform a pre-treatment complete blood count (CBC) and monitor CBCs every 2 to 4 weeks until doses are stabilized, and then as clinically indicated
- Manage thrombocytopenia by reducing the dose or temporarily interrupting Jakafi. Platelet transfusions may be necessary
- Patients developing anemia may require blood transfusions and/or dose modifications of Jakafi
- Severe neutropenia (ANC <0.5 × 109/L) was generally reversible by withholding Jakafi until recovery
- Serious bacterial, mycobacterial, fungal and viral infections have occurred. Delay starting Jakafi until active serious infections have resolved. Observe patients receiving Jakafi for signs and symptoms of infection and manage promptly. Use active surveillance and prophylactic antibiotics according to clinical guidelines
- Tuberculosis (TB) infection has been reported. Observe patients taking Jakafi for signs and symptoms of active TB and manage promptly. Prior to initiating Jakafi, evaluate patients for TB risk factors and test those at higher risk for latent infection. Consult a physician with expertise in the treatment of TB before starting Jakafi in patients with evidence of active or latent TB. Continuation of Jakafi during treatment of active TB should be based on the overall risk-benefit determination
- Progressive multifocal leukoencephalopathy (PML) has occurred with Jakafi treatment. If PML is suspected, stop Jakafi and evaluate
- Herpes zoster infection has been reported in patients receiving Jakafi. Advise patients about early signs and symptoms of herpes zoster and to seek early treatment. Herpes simplex virus reactivation and/or dissemination has been reported in patients receiving Jakafi. Monitor patients for the development of herpes simplex infections. If a patient develops evidence of dissemination of herpes simplex, consider interrupting treatment with Jakafi; patients should be promptly treated and monitored according to clinical guidelines
- Increases in hepatitis B viral load with or without associated elevations in alanine aminotransferase and aspartate aminotransferase have been reported in patients with chronic hepatitis B virus (HBV) infections. Monitor and treat patients with chronic HBV infection according to clinical guidelines
- When discontinuing Jakafi, myeloproliferative neoplasm-related symptoms may return within one week. After discontinuation, some patients with myelofibrosis have experienced fever, respiratory distress, hypotension, DIC, or multi-organ failure. If any of these occur after discontinuation or while tapering Jakafi, evaluate and treat any intercurrent illness and consider restarting or increasing the dose of Jakafi. Instruct patients not to interrupt or discontinue Jakafi without consulting their physician. When discontinuing or interrupting Jakafi for reasons other than thrombocytopenia or neutropenia, consider gradual tapering rather than abrupt discontinuation
- Non-melanoma skin cancers (NMSC) including basal cell, squamous cell, and Merkel cell carcinoma have occurred. Perform periodic skin examinations
- Treatment with Jakafi has been associated with increases in total cholesterol, low-density lipoprotein cholesterol, and triglycerides. Assess lipid parameters 8-12 weeks after initiating Jakafi. Monitor and treat according to clinical guidelines for the management of hyperlipidemia
- Another JAK-inhibitor has increased the risk of major adverse cardiovascular events (MACE), including cardiovascular death, myocardial infarction, and stroke (compared to those treated with tumor TNF blockers) in patients with rheumatoid arthritis, a condition for which Jakafi is not indicated. Consider the benefits and risks for the individual patient prior to initiating or continuing therapy with Jakafi particularly in patients who are current or past smokers and patients with other cardiovascular risk factors. Patients should be informed about the symptoms of serious cardiovascular events and the steps to take if they occur
- Another JAK-inhibitor has increased the risk of thrombosis, including deep venous thrombosis (DVT), pulmonary embolism (PE), and arterial thrombosis (compared to those treated with TNF blockers) in patients with rheumatoid arthritis, a condition for which Jakafi is not indicated. In patients with myelofibrosis (MF) and polycythemia vera (PV) treated with Jakafi in clinical trials, the rates of thromboembolic events were similar in Jakafi and control treated patients. Patients with symptoms of thrombosis should be promptly evaluated and treated appropriately
- Another JAK-inhibitor has increased the risk of lymphoma and other malignancies excluding NMSC (compared to those treated with TNF blockers) in patients with rheumatoid arthritis, a condition for which Jakafi is not indicated. Patients who are current or past smokers are at additional increased risk. Consider the benefits and risks for the individual patient prior to initiating or continuing therapy with Jakafi, particularly in patients with a known secondary malignancy (other than a successfully treated NMSC), patients who develop a malignancy, and patients who are current or past smokers
- In myelofibrosis and polycythemia vera, the most common nonhematologic adverse reactions (incidence ≥15%) were bruising, dizziness, headache, and diarrhea. In acute graft-versus-host disease, the most common nonhematologic adverse reactions (incidence >50%) were infections (pathogen not specified) and edema. In chronic graft-versus-host disease, the most common nonhematologic adverse reactions (incidence >20%) were infections (pathogen not specified) and viral infections
- Avoid concomitant use with fluconazole doses greater than 200 mg. Dose modifications may be required when administering Jakafi with fluconazole doses of 200 mg or less, or with strong CYP3A4 inhibitors, or in patients with renal or hepatic impairment. Patients should be closely monitored and the dose titrated based on safety and efficacy
- Use of Jakafi during pregnancy is not recommended and should only be used if the potential benefit justifies the potential risk to the fetus. Women taking Jakafi should not breastfeed during treatment and for 2 weeks after the final dose
Please view Full Prescribing Information for Jakafi.
-
MAJIC-PV study results: WBC control and risk of thrombosis
Dr Claire Harrison discusses findings from the RESPONSE and MAJIC-PV studies, including data on the correlation between WBC control and thrombosis-free survival. -
MAJIC-PV study results: Hct control and risk of thrombosis
Dr Claire Harrison discusses results from the RESPONSE and MAJIC-PV studies, including data on Hct and thrombosis-free survival. -
Durable Hct Control in Patients With PV
Hematologist-oncologist Dr Andrew Kuykendall discusses maintaining strict Hct control and when it may be time to intervene with Jakafi. -
Controlling Hct and Assessing Symptoms in Patients with PV
Hematologist-oncologist Dr Andrew Kuykendall details how he uncovers symptoms in patients with PV, and when it may be time to intervene with Jakafi. -
Controlling Hct and Assessing Symptoms in Patients With Polycythemia Vera
Hematologist-oncologist Dr Ruben Mesa discusses the importance of targeting optimal blood counts, assessing disease-related symptoms, and understanding when it may be the right time to intervene with Jakafi. -
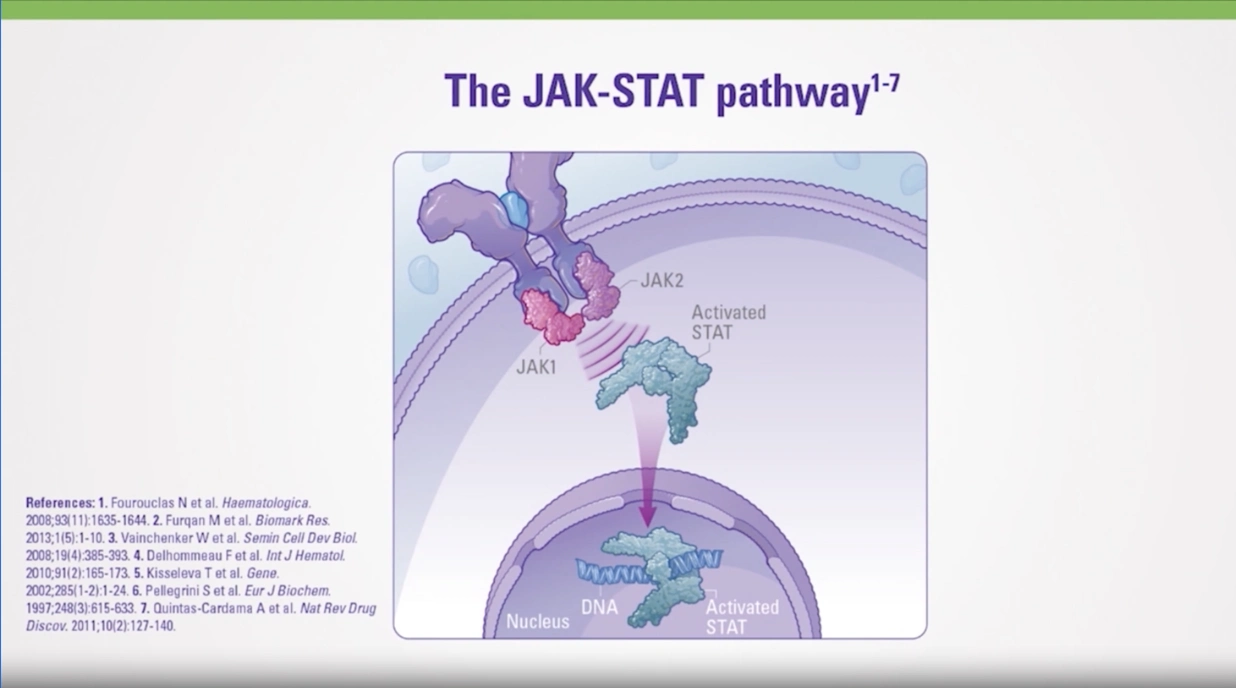
Mechanism of Action of Jakafi
Hematology specialist Dr Harry Erba reviews the mechanism of action of Jakafi, a JAK1 and JAK2 inhibitor, highlighting how Jakafi works to inhibit overactive JAK pathway signaling. Dr Erba also discusses safety data from the RESPONSE trial, which compared Jakafi to BAT for patients with PV who were either intolerant of or had an inadequate response to HU. -
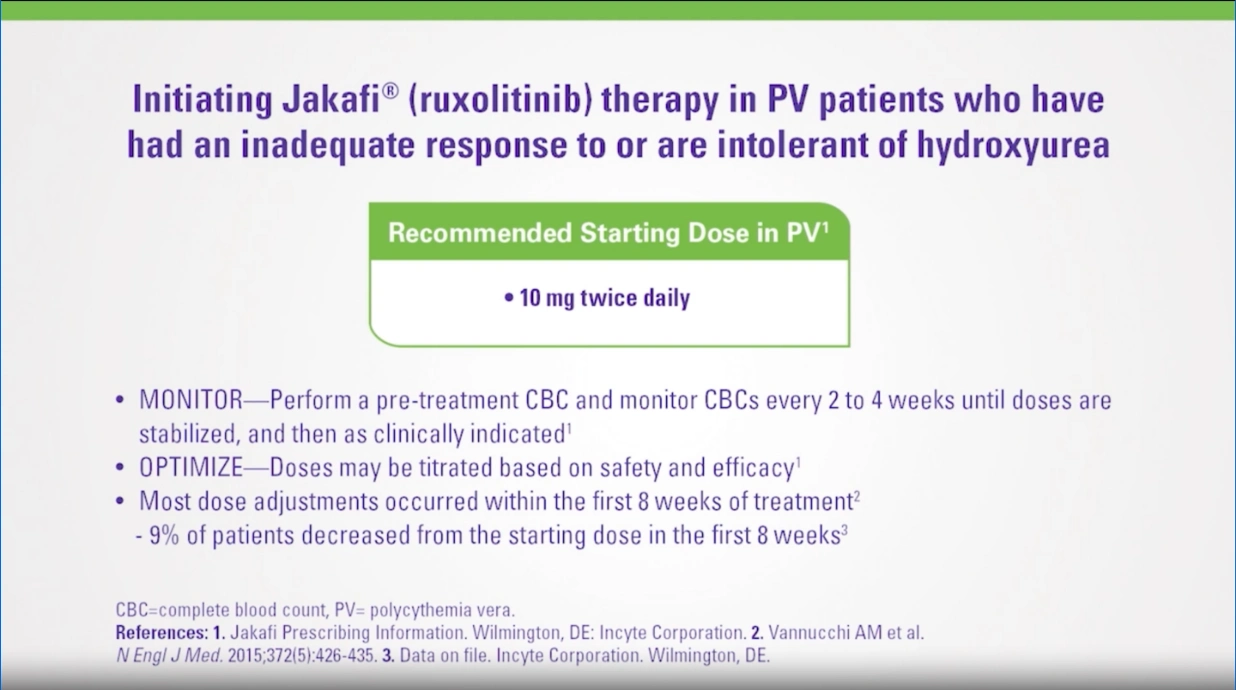
Dosing of Jakafi in Patients With PV Who Have Had an Inadequate Response to or Are Intolerant of HU
Hematology specialist Dr Harry Erba discusses the appropriate dosing of Jakafi in patients with PV who have had an inadequate response to or are intolerant of HU. Dr Erba addresses the recommended starting dose, dose reductions based on hemoglobin levels and/or platelet counts, and dose modifications needed because of insufficient response in PV.
BAT=best available therapy; Hct=hematocrit; HU=hydroxyurea; JAK=janus kinase; PV=polycythemia vera; RESPONSE=Randomized study of Efficacy and Safety in POlycythemia vera with JAK iNhibitor ruxolitinib verSus bEst available care; WBC=white blood cell.
INDICATIONS AND USAGE
JAKAFI®/JAKAFI XR™ (ruxolitinib) is for treatment of intermediate or high-risk myelofibrosis (MF), including primary MF, post–polycythemia vera MF and post–essential thrombocythemia MF in adults.
JAKAFI/JAKAFI XR is for treatment of polycythemia vera (PV) in adults who have had an inadequate response to or are intolerant of hydroxyurea.
JAKAFI/JAKAFI XR is for treatment of steroid-refractory acute graft-versus-host disease (aGVHD) in adult and pediatric patients 12 years and older.
JAKAFI/JAKAFI XR is for treatment of chronic graft-versus-host disease (cGVHD) after failure of one or two lines of systemic therapy in adult and pediatric patients 12 years and older.
IMPORTANT SAFETY INFORMATION
Warnings and Precautions
Thrombocytopenia, Anemia and Neutropenia
- JAKAFI/JAKAFI XR can cause dose-related effects of thrombocytopenia, anemia and neutropenia. Perform a pre-treatment complete blood count (CBC) and monitor CBCs every 2 to 4 weeks until doses are stabilized, and then as clinically indicated.
- Manage thrombocytopenia by reducing the dose or temporarily interrupting JAKAFI/JAKAFI XR. Platelet transfusions may be necessary.
- Patients developing anemia may require blood transfusions and/or dose modifications of JAKAFI/JAKAFI XR.
- Severe neutropenia (ANC <0.5 × 109/L) was generally reversible by withholding JAKAFI/JAKAFI XR until recovery.
Risk of Infection
Tuberculosis
- Serious bacterial, mycobacterial, fungal and viral infections have occurred. Delay starting JAKAFI/JAKAFI XR until active serious infections have resolved. Observe patients receiving JAKAFI/JAKAFI XR for signs and symptoms of infection and manage promptly.
- Tuberculosis (TB) infection with JAKAFI/JAKAFI XR has been reported. Observe patients taking JAKAFI/JAKAFI XR for signs and symptoms of active TB and manage promptly. Prior to initiating, evaluate patients for TB risk factors and test those at higher risk for latent infection. Consult a physician with expertise in the treatment of TB before starting in patients with evidence of active or latent TB. Continuation during treatment of active TB should be based on the overall risk-benefit determination.
Progressive Multifocal Leukoencephalopathy
- Progressive multifocal leukoencephalopathy (PML) has occurred with JAKAFI/JAKAFI XR treatment. If PML is suspected, stop JAKAFI/JAKAFI XR and evaluate.
Herpes Zoster and Herpes Simplex
- Herpes zoster infection, reactivation and/or dissemination has been reported in patients receiving JAKAFI/JAKAFI XR. Advise patients about early signs and symptoms of herpes zoster and seek treatment. Monitor patients for the development of herpes simplex infections. If a patient develops evidence of dissemination of herpes simplex, consider interrupting treatment.
Hepatitis B
- Increases in hepatitis B viral load with or without associated elevations in alanine aminotransferase and aspartate aminotransferase have been reported in patients with chronic hepatitis B virus (HBV) infections.
Symptom Exacerbation Following Interruption or Discontinuation of Treatment
- When discontinuing JAK-Inhibitors, including JAKAFI/JAKAFI XR, myeloproliferative neoplasm-related signs and symptoms may flare. After discontinuation, some patients with myelofibrosis have experienced fever, respiratory distress, hypotension, disseminated intravascular coagulation (DIC), or multi-organ failure. If any of these occur after discontinuation or while tapering JAKAFI/JAKAFI XR, evaluate and treat any intercurrent illness and consider restarting or increasing the dose. Instruct patients not to interrupt or discontinue JAKAFI/JAKAFI XR without consulting their physician. When discontinuing or interrupting JAKAFI/JAKAFI XR for reasons other than life-threatening toxicities, consider gradual tapering rather than abrupt discontinuation.
Non-Melanoma Skin Cancer (NMSC)
- NMSC including basal cell, squamous cell, and Merkel cell carcinoma have occurred. Perform periodic skin examinations.
Lipid Elevations
- Treatment with JAKAFI/JAKAFI XR has been associated with increases in total cholesterol, low-density lipoprotein cholesterol, and triglycerides. Assess lipid parameters 8-12 weeks after initiation.
Major Adverse Cardiovascular Events (MACE)
- Another JAK-inhibitor has increased the risk of major adverse cardiovascular events (MACE), including cardiovascular death, myocardial infarction, and stroke (compared to those treated with TNF blockers), in patients with rheumatoid arthritis, a condition for which JAKAFI/JAKAFI XR is not indicated. Consider the benefits and risks for the individual patient prior to initiating or continuing therapy, particularly in patients who are current or past smokers and patients with other cardiovascular risk factors. Patients should be informed about the symptoms of serious cardiovascular events and the steps to take if they occur.
Thrombosis
- Another JAK-inhibitor has increased the risk of thrombosis, including deep venous thrombosis (DVT), pulmonary embolism (PE), and arterial thrombosis (compared to those treated with TNF blockers), in patients with rheumatoid arthritis, a condition for which JAKAFI/JAKAFI XR is not indicated. In patients with myelofibrosis (MF) and polycythemia vera (PV), the rates of thromboembolic events were similar in JAKAFI/JAKAFI XR and control treated patients. Patients with symptoms of thrombosis should be promptly evaluated and treated appropriately.
Secondary Malignancies
- Another JAK-inhibitor has increased the risk of lymphoma and other malignancies, excluding NMSC (compared to those treated with TNF blockers), in patients with rheumatoid arthritis, a condition for which JAKAFI/JAKAFI XR is not indicated. Patients who are current or past smokers are at additional increased risk.
Adverse Reactions
- In myelofibrosis, the most common hematologic adverse reactions (incidence >20%) were thrombocytopenia and anemia. The most common nonhematologic adverse reactions (incidence ≥15%) were bruising, dizziness, headache and diarrhea.
- In polycythemia vera, the most common hematologic adverse reactions (incidence >20%) were thrombocytopenia and anemia. The most common nonhematologic adverse reactions (incidence ≥15%) were bruising, dizziness, headache and diarrhea.
- In acute graft-versus-host disease, the most common hematologic adverse reactions (incidence >50%) were anemia, thrombocytopenia and neutropenia. The most common nonhematologic adverse reactions (incidence >50%) were infections (pathogen not specified) and edema.
- In chronic graft-versus-host disease, the most common hematologic adverse reactions (incidence >35%) were anemia and thrombocytopenia. The most common nonhematologic adverse reactions (incidence ≥20%) were infections (pathogen not specified) and viral infections.
Drug Interactions
- Avoid concomitant use with fluconazole doses greater than 200 mg. Dose modifications may be required when administering fluconazole doses of 200 mg or less, or with strong CYP3A4 inhibitors, or in patients with renal or hepatic impairment. Patients should be closely monitored and the dose titrated based on safety and efficacy.
Pregnancy
- Use during pregnancy is not recommended and should only be used if the potential benefit justifies the potential risk to the fetus. Women taking JAKAFI/JAKAFI XR should not breastfeed during treatment and for 2 weeks after the final dose.
Please see Full Prescribing Information for JAKAFI and JAKAFI XR.
INDICATIONS AND USAGE
JAKAFI®/JAKAFI XR™ (ruxolitinib) is for treatment of intermediate or high-risk myelofibrosis (MF), including primary MF, post–polycythemia vera MF and post–essential thrombocythemia MF in adults.
JAKAFI/JAKAFI XR is for treatment of polycythemia vera (PV) in adults who have had an inadequate response to or are intolerant of hydroxyurea.
JAKAFI/JAKAFI XR is for treatment of steroid-refractory acute graft-versus-host disease (aGVHD) in adult and pediatric patients 12 years and older.
JAKAFI/JAKAFI XR is for treatment of chronic graft-versus-host disease (cGVHD) after failure of one or two lines of systemic therapy in adult and pediatric patients 12 years and older.
IMPORTANT SAFETY INFORMATION
Warnings and Precautions
Thrombocytopenia, Anemia and Neutropenia
- JAKAFI/JAKAFI XR can cause dose-related effects of thrombocytopenia, anemia and neutropenia. Perform a pre-treatment complete blood count (CBC) and monitor CBCs every 2 to 4 weeks until doses are stabilized, and then as clinically indicated.
- Manage thrombocytopenia by reducing the dose or temporarily interrupting JAKAFI/JAKAFI XR. Platelet transfusions may be necessary.
- Patients developing anemia may require blood transfusions and/or dose modifications of JAKAFI/JAKAFI XR.
- Severe neutropenia (ANC <0.5 × 109/L) was generally reversible by withholding JAKAFI/JAKAFI XR until recovery.
Risk of Infection
Tuberculosis
- Serious bacterial, mycobacterial, fungal and viral infections have occurred. Delay starting JAKAFI/JAKAFI XR until active serious infections have resolved. Observe patients receiving JAKAFI/JAKAFI XR for signs and symptoms of infection and manage promptly.
- Tuberculosis (TB) infection with JAKAFI/JAKAFI XR has been reported. Observe patients taking JAKAFI/JAKAFI XR for signs and symptoms of active TB and manage promptly. Prior to initiating, evaluate patients for TB risk factors and test those at higher risk for latent infection. Consult a physician with expertise in the treatment of TB before starting in patients with evidence of active or latent TB. Continuation during treatment of active TB should be based on the overall risk-benefit determination.
Progressive Multifocal Leukoencephalopathy
- Progressive multifocal leukoencephalopathy (PML) has occurred with JAKAFI/JAKAFI XR treatment. If PML is suspected, stop JAKAFI/JAKAFI XR and evaluate.
Herpes Zoster and Herpes Simplex
- Herpes zoster infection, reactivation and/or dissemination has been reported in patients receiving JAKAFI/JAKAFI XR. Advise patients about early signs and symptoms of herpes zoster and seek treatment. Monitor patients for the development of herpes simplex infections. If a patient develops evidence of dissemination of herpes simplex, consider interrupting treatment.
Hepatitis B
- Increases in hepatitis B viral load with or without associated elevations in alanine aminotransferase and aspartate aminotransferase have been reported in patients with chronic hepatitis B virus (HBV) infections.
Symptom Exacerbation Following Interruption or Discontinuation of Treatment
- When discontinuing JAK-Inhibitors, including JAKAFI/JAKAFI XR, myeloproliferative neoplasm-related signs and symptoms may flare. After discontinuation, some patients with myelofibrosis have experienced fever, respiratory distress, hypotension, disseminated intravascular coagulation (DIC), or multi-organ failure. If any of these occur after discontinuation or while tapering JAKAFI/JAKAFI XR, evaluate and treat any intercurrent illness and consider restarting or increasing the dose. Instruct patients not to interrupt or discontinue JAKAFI/JAKAFI XR without consulting their physician. When discontinuing or interrupting JAKAFI/JAKAFI XR for reasons other than life-threatening toxicities, consider gradual tapering rather than abrupt discontinuation.
Non-Melanoma Skin Cancer (NMSC)
- NMSC including basal cell, squamous cell, and Merkel cell carcinoma have occurred. Perform periodic skin examinations.
Lipid Elevations
- Treatment with JAKAFI/JAKAFI XR has been associated with increases in total cholesterol, low-density lipoprotein cholesterol, and triglycerides. Assess lipid parameters 8-12 weeks after initiation.
Major Adverse Cardiovascular Events (MACE)
- Another JAK-inhibitor has increased the risk of major adverse cardiovascular events (MACE), including cardiovascular death, myocardial infarction, and stroke (compared to those treated with TNF blockers), in patients with rheumatoid arthritis, a condition for which JAKAFI/JAKAFI XR is not indicated. Consider the benefits and risks for the individual patient prior to initiating or continuing therapy, particularly in patients who are current or past smokers and patients with other cardiovascular risk factors. Patients should be informed about the symptoms of serious cardiovascular events and the steps to take if they occur.
Thrombosis
- Another JAK-inhibitor has increased the risk of thrombosis, including deep venous thrombosis (DVT), pulmonary embolism (PE), and arterial thrombosis (compared to those treated with TNF blockers), in patients with rheumatoid arthritis, a condition for which JAKAFI/JAKAFI XR is not indicated. In patients with myelofibrosis (MF) and polycythemia vera (PV), the rates of thromboembolic events were similar in JAKAFI/JAKAFI XR and control treated patients. Patients with symptoms of thrombosis should be promptly evaluated and treated appropriately.
Secondary Malignancies
- Another JAK-inhibitor has increased the risk of lymphoma and other malignancies, excluding NMSC (compared to those treated with TNF blockers), in patients with rheumatoid arthritis, a condition for which JAKAFI/JAKAFI XR is not indicated. Patients who are current or past smokers are at additional increased risk.
Adverse Reactions
- In myelofibrosis, the most common hematologic adverse reactions (incidence >20%) were thrombocytopenia and anemia. The most common nonhematologic adverse reactions (incidence ≥15%) were bruising, dizziness, headache and diarrhea.
- In polycythemia vera, the most common hematologic adverse reactions (incidence >20%) were thrombocytopenia and anemia. The most common nonhematologic adverse reactions (incidence ≥15%) were bruising, dizziness, headache and diarrhea.
- In acute graft-versus-host disease, the most common hematologic adverse reactions (incidence >50%) were anemia, thrombocytopenia and neutropenia. The most common nonhematologic adverse reactions (incidence >50%) were infections (pathogen not specified) and edema.
- In chronic graft-versus-host disease, the most common hematologic adverse reactions (incidence >35%) were anemia and thrombocytopenia. The most common nonhematologic adverse reactions (incidence ≥20%) were infections (pathogen not specified) and viral infections.
Drug Interactions
- Avoid concomitant use with fluconazole doses greater than 200 mg. Dose modifications may be required when administering fluconazole doses of 200 mg or less, or with strong CYP3A4 inhibitors, or in patients with renal or hepatic impairment. Patients should be closely monitored and the dose titrated based on safety and efficacy.
Pregnancy
- Use during pregnancy is not recommended and should only be used if the potential benefit justifies the potential risk to the fetus. Women taking JAKAFI/JAKAFI XR should not breastfeed during treatment and for 2 weeks after the final dose.
Please see Full Prescribing Information for JAKAFI and JAKAFI XR.