Perspectives and insights from PV experts
The resources on this page offer information and insights about Jakafi® (ruxolitinib) and treatment of patients with PV who have had an inadequate response to or are intolerant of HU. Be sure to check back regularly as new materials will be added as they become available.


Controlling Hct and Assessing Symptoms in Patients With Polycythemia Vera
Hematologist-oncologist Dr Ruben Mesa discusses the importance of targeting optimal blood counts, assessing disease-related symptoms, and understanding when it may be the right time to intervene with Jakafi.
Hi, my name is Dr Ruben Mesa and I'm a hematologic oncologist.
Today, I’d like to talk to you about the importance of monitoring blood counts in patients with PV, or polycythemia vera, and how I assess for disease‐related symptoms, as symptoms are an important indicator of disease progression and can easily be overlooked.
My primary goal when managing patients with PV is to obtain optimal hematocrit control of less than 45%.
For patients with PV, we know that suboptimal control of hematocrit, which is anything greater than 45%, is associated with significant risks, even if the hematocrit is 47 or 48%. So, to protect my patients, I typically intervene slightly below 45%.
Oftentimes, I find that hydroxyurea may not be optimal for all of my patients. When I see a patient who requires more than 4 phlebotomies per year while on the maximum tolerated dose of hydroxyurea, that suggests to me that they have a more proliferative disease and a switch in cytoreductive therapy may be necessary.
I also try to understand the symptoms patients may be experiencing with their disease to get an accurate assessment of how they’re feeling.
In my experience, patients with PV can experience significant symptom burden, despite being on hydroxyurea.
I find that patients often try to downplay symptoms because they worry about not having enough time during the visit or they don’t want to come across as complaining about their disease.
So, to make sure I get accurate responses, I ask specific questions about key disease-related symptoms such as, “Are you having night sweats?” “Are you having itching?” or “Are you having pain anywhere?” Fatigue may be more challenging to assess so I ask more specifically about energy levels. I’m careful to not overlook symptoms because they can be an important indicator of disease progression.
In my clinical experience, hydroxyurea may not always address key disease‐related symptoms such as fatigue, itching, or night sweats and may not provide durable hematocrit control.
Instead, for my appropriate patients with PV, I aim for a therapy that demonstrates effective hematocrit control. And for these patients, Jakafi is my treatment of choice.
My confidence in prescribing Jakafi comes from the results of the RESPONSE trial, as the study was designed to evaluate Jakafi vs BAT in controlling hematocrit and spleen volume. In addition to that, an exploratory analysis was done in this study that looked very specifically at patient self‐reported symptom scores.
It was a phase 3 trial that enrolled patients with polycythemia vera who were resistant to, or intolerant of, hydroxyurea, and required phlebotomy for hematocrit control.
To meet hematocrit control criteria, patients could not have received phlebotomy between weeks 8 and 32.
The study found that 23% of patients on Jakafi achieved the composite primary endpoint of hematocrit control and spleen volume reduction of at least 35% at week 32, compared to less than 1% in the BAT arm.
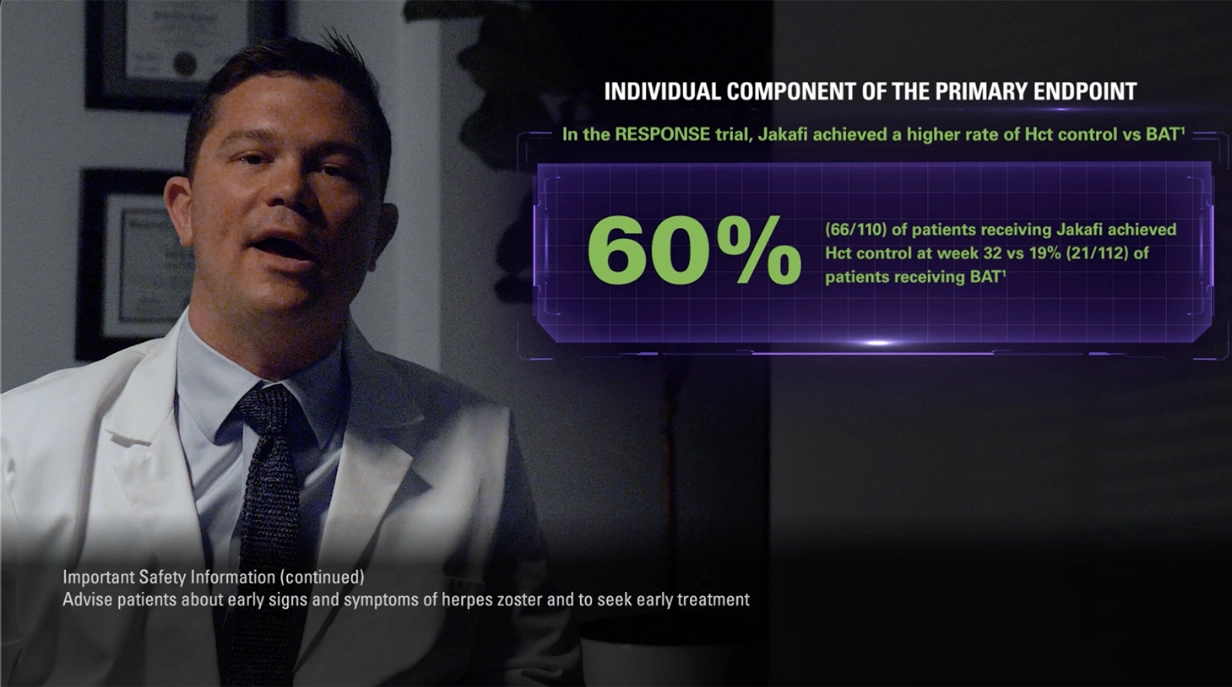
Looking at just the hematocrit response, 60% of patients on Jakafi achieved hematocrit control compared with only 19% of patients on BAT.
And in that BAT arm, it’s important to note that 60% of the patients were on hydroxyurea.
These data give me the confidence to initiate Jakafi in my patients with PV who are unable to achieve hematocrit control below 45%, despite being on the maximum tolerated dose of hydroxyurea and phlebotomy.
The RESPONSE trial also looked at reduction of symptoms. In this exploratory endpoint, 49% of patients on Jakafi reported at least 50% reduction in the total symptom score.
Now, we know that RESPONSE was an open‐label trial and therefore was not designed to evaluate differences in symptoms.
Based on the exploratory endpoint, patients receiving Jakafi had reductions in all symptom clusters reported. Cytokine-related symptoms included those such as fatigue, itching, and night sweats. Hyperviscosity symptoms included headache, dizziness, and paresthesia, while splenomegaly symptoms included early satiety and abdominal discomfort.
So, for my patients with elevated hematocrit levels who are still experiencing disease‐related symptoms, it’s important to determine when a switch in therapy may be appropriate.
The results from the RESPONSE trial, along with my own clinical experience, give me the confidence to prescribe Jakafi in my appropriate patients with polycythemia vera who have had an inadequate response to or are intolerant of hydroxyurea.
So, when I have patients who are unable to achieve hematocrit control below 45%, and are experiencing symptoms such as fatigue, pruritus, or night sweats, this tells me that hydroxyurea is no longer sufficient. And that’s when I typically intervene with Jakafi.
Let’s review the safety information for Jakafi.
INDICATIONS AND USAGE
Jakafi is indicated for treatment of polycythemia vera (PV) in adults who have had an inadequate response to or are intolerant of hydroxyurea.
IMPORTANT SAFETY INFORMATION
- Treatment with Jakafi® (ruxolitinib) can cause thrombocytopenia, anemia and neutropenia, which are each dose-related effects. Perform a pre-treatment complete blood count (CBC) and monitor CBCs every 2 to 4 weeks until doses are stabilized, and then as clinically indicated
- Manage thrombocytopenia by reducing the dose or temporarily interrupting Jakafi. Platelet transfusions may be necessary
- Patients developing anemia may require blood transfusions and/or dose modifications of Jakafi
- Severe neutropenia (ANC <0.5 × 109/L) was generally reversible by withholding Jakafi until recovery
- Serious bacterial, mycobacterial, fungal and viral infections have occurred. Delay starting Jakafi until active serious infections have resolved. Observe patients receiving Jakafi for signs and symptoms of infection and manage promptly. Use active surveillance and prophylactic antibiotics according to clinical guidelines
- Tuberculosis (TB) infection has been reported. Observe patients taking Jakafi for signs and symptoms of active TB and manage promptly. Prior to initiating Jakafi, evaluate patients for TB risk factors and test those at higher risk for latent infection. Consult a physician with expertise in the treatment of TB before starting Jakafi in patients with evidence of active or latent TB. Continuation of Jakafi during treatment of active TB should be based on the overall risk-benefit determination
- Progressive multifocal leukoencephalopathy (PML) has occurred with Jakafi treatment. If PML is suspected, stop Jakafi and evaluate
- Herpes zoster infection has been reported in patients receiving Jakafi. Advise patients about early signs and symptoms of herpes zoster and to seek early treatment. Herpes simplex virus reactivation and/or dissemination has been reported in patients receiving Jakafi. Monitor patients for the development of herpes simplex infections. If a patient develops evidence of dissemination of herpes simplex, consider interrupting treatment with Jakafi; patients should be promptly treated and monitored according to clinical guidelines
- Increases in hepatitis B viral load with or without associated elevations in alanine aminotransferase and aspartate aminotransferase have been reported in patients with chronic hepatitis B virus (HBV) infections. Monitor and treat patients with chronic HBV infection according to clinical guidelines
- When discontinuing Jakafi, myeloproliferative neoplasm-related symptoms may return within one week. After discontinuation, some patients with myelofibrosis have experienced fever, respiratory distress, hypotension, DIC, or multi-organ failure. If any of these occur after discontinuation or while tapering Jakafi, evaluate and treat any intercurrent illness and consider restarting or increasing the dose of Jakafi. Instruct patients not to interrupt or discontinue Jakafi without consulting their physician. When discontinuing or interrupting Jakafi for reasons other than thrombocytopenia or neutropenia, consider gradual tapering rather than abrupt discontinuation
- Non-melanoma skin cancers (NMSC) including basal cell, squamous cell, and Merkel cell carcinoma have occurred. Perform periodic skin examinations
- Treatment with Jakafi has been associated with increases in total cholesterol, low-density lipoprotein cholesterol, and triglycerides. Assess lipid parameters 8-12 weeks after initiating Jakafi. Monitor and treat according to clinical guidelines for the management of hyperlipidemia
- Another JAK-inhibitor has increased the risk of major adverse cardiovascular events (MACE), including cardiovascular death, myocardial infarction, and stroke (compared to those treated with tumor TNF blockers) in patients with rheumatoid arthritis, a condition for which Jakafi is not indicated. Consider the benefits and risks for the individual patient prior to initiating or continuing therapy with Jakafi particularly in patients who are current or past smokers and patients with other cardiovascular risk factors. Patients should be informed about the symptoms of serious cardiovascular events and the steps to take if they occur
- Another JAK-inhibitor has increased the risk of thrombosis, including deep venous thrombosis (DVT), pulmonary embolism (PE), and arterial thrombosis (compared to those treated with TNF blockers) in patients with rheumatoid arthritis, a condition for which Jakafi is not indicated. In patients with myelofibrosis (MF) and polycythemia vera (PV) treated with Jakafi in clinical trials, the rates of thromboembolic events were similar in Jakafi and control treated patients. Patients with symptoms of thrombosis should be promptly evaluated and treated appropriately
- Another JAK-inhibitor has increased the risk of lymphoma and other malignancies excluding NMSC (compared to those treated with TNF blockers) in patients with rheumatoid arthritis, a condition for which Jakafi is not indicated. Patients who are current or past smokers are at additional increased risk. Consider the benefits and risks for the individual patient prior to initiating or continuing therapy with Jakafi, particularly in patients with a known secondary malignancy (other than a successfully treated NMSC), patients who develop a malignancy, and patients who are current or past smokers
- In myelofibrosis and polycythemia vera, the most common nonhematologic adverse reactions (incidence ≥15%) were bruising, dizziness, headache, and diarrhea. In acute graft-versus-host disease, the most common nonhematologic adverse reactions (incidence >50%) were infections (pathogen not specified) and edema. In chronic graft-versus-host disease, the most common nonhematologic adverse reactions (incidence >20%) were infections (pathogen not specified) and viral infections
- Avoid concomitant use with fluconazole doses greater than 200 mg. Dose modifications may be required when administering Jakafi with fluconazole doses of 200 mg or less, or with strong CYP3A4 inhibitors, or in patients with renal or hepatic impairment. Patients should be closely monitored and the dose titrated based on safety and efficacy
- Use of Jakafi during pregnancy is not recommended and should only be used if the potential benefit justifies the potential risk to the fetus. Women taking Jakafi should not breastfeed during treatment and for 2 weeks after the final dose
Please see Full Prescribing Information for Jakafi.
-

MAJIC-PV study results: WBC control and risk of thrombosis
Dr Claire Harrison discusses findings from the RESPONSE and MAJIC-PV studies, including data on the correlation between WBC control and thrombosis-free survival. -

MAJIC-PV study results: Hct control and risk of thrombosis
Dr Claire Harrison discusses results from the RESPONSE and MAJIC-PV studies, including data on Hct and thrombosis-free survival. -

Hct Control and WBC Reduction in Patients With PV
Hematologist-oncologist Dr Andrew Kuykendall shares how he manages progressive WBC counts and when it may be time to intervene with Jakafi. -
Durable Hct Control in Patients With PV
Hematologist-oncologist Dr Andrew Kuykendall discusses maintaining strict Hct control and when it may be time to intervene with Jakafi. -

Controlling Hct and Assessing Symptoms in Patients with PV
Hematologist-oncologist Dr Andrew Kuykendall details how he uncovers symptoms in patients with PV, and when it may be time to intervene with Jakafi. -

Mechanism of Action of Jakafi
Hematology specialist Dr Harry Erba reviews the mechanism of action of Jakafi, a JAK1 and JAK2 inhibitor, highlighting how Jakafi works to inhibit overactive JAK pathway signaling. Dr Erba also discusses safety data from the RESPONSE trial, which compared Jakafi to BAT for patients with PV who were either intolerant of or had an inadequate response to HU. -

Dosing of Jakafi in Patients With PV Who Have Had an Inadequate Response to or Are Intolerant of HU
Hematology specialist Dr Harry Erba discusses the appropriate dosing of Jakafi in patients with PV who have had an inadequate response to or are intolerant of HU. Dr Erba addresses the recommended starting dose, dose reductions based on hemoglobin levels and/or platelet counts, and dose modifications needed because of insufficient response in PV.
BAT=best available therapy; Hct=hematocrit; HU=hydroxyurea; JAK=janus kinase; PV=polycythemia vera; RESPONSE=Randomized study of Efficacy and Safety in POlycythemia vera with JAK iNhibitor ruxolitinib verSus bEst available care; WBC=white blood cell.
Indications and Usage
Jakafi® (ruxolitinib) is indicated for treatment of polycythemia vera (PV) in adults who have had an inadequate response to or are intolerant of hydroxyurea.
Jakafi is indicated for treatment of intermediate or high-risk myelofibrosis (MF), including primary MF, post–polycythemia vera MF and post–essential thrombocythemia MF in adults.
Jakafi is indicated for treatment of steroid-refractory acute graft-versus-host disease (aGVHD) in adult and pediatric patients 12 years and older.
Jakafi is indicated for treatment of chronic graft-versus-host disease (cGVHD) after failure of one or two lines of systemic therapy in adult and pediatric patients 12 years and older.
Important Safety Information
- Treatment with Jakafi can cause thrombocytopenia, anemia and neutropenia, which are each dose-related effects. Perform a pre-treatment complete blood count (CBC) and monitor CBCs every 2 to 4 weeks until doses are stabilized, and then as clinically indicated
- Manage thrombocytopenia by reducing the dose or temporarily interrupting Jakafi. Platelet transfusions may be necessary
- Patients developing anemia may require blood transfusions and/or dose modifications of Jakafi
- Severe neutropenia (ANC <0.5 × 109/L) was generally reversible by withholding Jakafi until recovery
- Serious bacterial, mycobacterial, fungal and viral infections have occurred. Delay starting Jakafi until active serious infections have resolved. Observe patients receiving Jakafi for signs and symptoms of infection and manage promptly. Use active surveillance and prophylactic antibiotics according to clinical guidelines
- Tuberculosis (TB) infection has been reported. Observe patients taking Jakafi for signs and symptoms of active TB and manage promptly. Prior to initiating Jakafi, evaluate patients for TB risk factors and test those at higher risk for latent infection. Consult a physician with expertise in the treatment of TB before starting Jakafi in patients with evidence of active or latent TB. Continuation of Jakafi during treatment of active TB should be based on the overall risk-benefit determination
- Progressive multifocal leukoencephalopathy (PML) has occurred with Jakafi treatment. If PML is suspected, stop Jakafi and evaluate
- Herpes zoster infection has been reported in patients receiving Jakafi. Advise patients about early signs and symptoms of herpes zoster and to seek early treatment. Herpes simplex virus reactivation and/or dissemination has been reported in patients receiving Jakafi. Monitor patients for the development of herpes simplex infections. If a patient develops evidence of dissemination of herpes simplex, consider interrupting treatment with Jakafi; patients should be promptly treated and monitored according to clinical guidelines
- Increases in hepatitis B viral load with or without associated elevations in alanine aminotransferase and aspartate aminotransferase have been reported in patients with chronic hepatitis B virus (HBV) infections. Monitor and treat patients with chronic HBV infection according to clinical guidelines
- When discontinuing Jakafi, myeloproliferative neoplasm-related symptoms may return within one week. After discontinuation, some patients with myelofibrosis have experienced fever, respiratory distress, hypotension, DIC, or multi-organ failure. If any of these occur after discontinuation or while tapering Jakafi, evaluate and treat any intercurrent illness and consider restarting or increasing the dose of Jakafi. Instruct patients not to interrupt or discontinue Jakafi without consulting their physician. When discontinuing or interrupting Jakafi for reasons other than thrombocytopenia or neutropenia, consider gradual tapering rather than abrupt discontinuation
- Non-melanoma skin cancers (NMSC) including basal cell, squamous cell, and Merkel cell carcinoma have occurred. Perform periodic skin examinations
- Treatment with Jakafi has been associated with increases in total cholesterol, low-density lipoprotein cholesterol, and triglycerides. Assess lipid parameters 8-12 weeks after initiating Jakafi. Monitor and treat according to clinical guidelines for the management of hyperlipidemia
- Another JAK-inhibitor has increased the risk of major adverse cardiovascular events (MACE), including cardiovascular death, myocardial infarction, and stroke (compared to those treated with tumor TNF blockers) in patients with rheumatoid arthritis, a condition for which Jakafi is not indicated. Consider the benefits and risks for the individual patient prior to initiating or continuing therapy with Jakafi particularly in patients who are current or past smokers and patients with other cardiovascular risk factors. Patients should be informed about the symptoms of serious cardiovascular events and the steps to take if they occur
- Another JAK-inhibitor has increased the risk of thrombosis, including deep venous thrombosis (DVT), pulmonary embolism (PE), and arterial thrombosis (compared to those treated with TNF blockers) in patients with rheumatoid arthritis, a condition for which Jakafi is not indicated. In patients with myelofibrosis (MF) and polycythemia vera (PV) treated with Jakafi in clinical trials, the rates of thromboembolic events were similar in Jakafi and control treated patients. Patients with symptoms of thrombosis should be promptly evaluated and treated appropriately
- Another JAK-inhibitor has increased the risk of lymphoma and other malignancies excluding NMSC (compared to those treated with TNF blockers) in patients with rheumatoid arthritis, a condition for which Jakafi is not indicated. Patients who are current or past smokers are at additional increased risk. Consider the benefits and risks for the individual patient prior to initiating or continuing therapy with Jakafi, particularly in patients with a known secondary malignancy (other than a successfully treated NMSC), patients who develop a malignancy, and patients who are current or past smokers
- In myelofibrosis and polycythemia vera, the most common nonhematologic adverse reactions (incidence ≥15%) were bruising, dizziness, headache, and diarrhea. In acute graft-versus-host disease, the most common nonhematologic adverse reactions (incidence >50%) were infections (pathogen not specified) and edema. In chronic graft-versus-host disease, the most common nonhematologic adverse reactions (incidence >20%) were infections (pathogen not specified) and viral infections
- Avoid concomitant use with fluconazole doses greater than 200 mg. Dose modifications may be required when administering Jakafi with fluconazole doses of 200 mg or less, or with strong CYP3A4 inhibitors, or in patients with renal or hepatic impairment. Patients should be closely monitored and the dose titrated based on safety and efficacy
- Use of Jakafi during pregnancy is not recommended and should only be used if the potential benefit justifies the potential risk to the fetus. Women taking Jakafi should not breastfeed during treatment and for 2 weeks after the final dose
Please see Full Prescribing Information for Jakafi.
Indications and Usage
Jakafi® (ruxolitinib) is indicated for treatment of polycythemia vera (PV) in adults who have had an inadequate response to or are intolerant of hydroxyurea.
Jakafi is indicated for treatment of intermediate or high-risk myelofibrosis (MF), including primary MF, post–polycythemia vera MF and post–essential thrombocythemia MF in adults.
Jakafi is indicated for treatment of steroid-refractory acute graft-versus-host disease (aGVHD) in adult and pediatric patients 12 years and older.
Jakafi is indicated for treatment of chronic graft-versus-host disease (cGVHD) after failure of one or two lines of systemic therapy in adult and pediatric patients 12 years and older.
Important Safety Information
- Treatment with Jakafi can cause thrombocytopenia, anemia and neutropenia, which are each dose-related effects. Perform a pre-treatment complete blood count (CBC) and monitor CBCs every 2 to 4 weeks until doses are stabilized, and then as clinically indicated
- Manage thrombocytopenia by reducing the dose or temporarily interrupting Jakafi. Platelet transfusions may be necessary
- Patients developing anemia may require blood transfusions and/or dose modifications of Jakafi
- Severe neutropenia (ANC <0.5 × 109/L) was generally reversible by withholding Jakafi until recovery
- Serious bacterial, mycobacterial, fungal and viral infections have occurred. Delay starting Jakafi until active serious infections have resolved. Observe patients receiving Jakafi for signs and symptoms of infection and manage promptly. Use active surveillance and prophylactic antibiotics according to clinical guidelines
- Tuberculosis (TB) infection has been reported. Observe patients taking Jakafi for signs and symptoms of active TB and manage promptly. Prior to initiating Jakafi, evaluate patients for TB risk factors and test those at higher risk for latent infection. Consult a physician with expertise in the treatment of TB before starting Jakafi in patients with evidence of active or latent TB. Continuation of Jakafi during treatment of active TB should be based on the overall risk-benefit determination
- Progressive multifocal leukoencephalopathy (PML) has occurred with Jakafi treatment. If PML is suspected, stop Jakafi and evaluate
- Herpes zoster infection has been reported in patients receiving Jakafi. Advise patients about early signs and symptoms of herpes zoster and to seek early treatment. Herpes simplex virus reactivation and/or dissemination has been reported in patients receiving Jakafi. Monitor patients for the development of herpes simplex infections. If a patient develops evidence of dissemination of herpes simplex, consider interrupting treatment with Jakafi; patients should be promptly treated and monitored according to clinical guidelines
- Increases in hepatitis B viral load with or without associated elevations in alanine aminotransferase and aspartate aminotransferase have been reported in patients with chronic hepatitis B virus (HBV) infections. Monitor and treat patients with chronic HBV infection according to clinical guidelines
- When discontinuing Jakafi, myeloproliferative neoplasm-related symptoms may return within one week. After discontinuation, some patients with myelofibrosis have experienced fever, respiratory distress, hypotension, DIC, or multi-organ failure. If any of these occur after discontinuation or while tapering Jakafi, evaluate and treat any intercurrent illness and consider restarting or increasing the dose of Jakafi. Instruct patients not to interrupt or discontinue Jakafi without consulting their physician. When discontinuing or interrupting Jakafi for reasons other than thrombocytopenia or neutropenia, consider gradual tapering rather than abrupt discontinuation
- Non-melanoma skin cancers (NMSC) including basal cell, squamous cell, and Merkel cell carcinoma have occurred. Perform periodic skin examinations
- Treatment with Jakafi has been associated with increases in total cholesterol, low-density lipoprotein cholesterol, and triglycerides. Assess lipid parameters 8-12 weeks after initiating Jakafi. Monitor and treat according to clinical guidelines for the management of hyperlipidemia
- Another JAK-inhibitor has increased the risk of major adverse cardiovascular events (MACE), including cardiovascular death, myocardial infarction, and stroke (compared to those treated with tumor TNF blockers) in patients with rheumatoid arthritis, a condition for which Jakafi is not indicated. Consider the benefits and risks for the individual patient prior to initiating or continuing therapy with Jakafi particularly in patients who are current or past smokers and patients with other cardiovascular risk factors. Patients should be informed about the symptoms of serious cardiovascular events and the steps to take if they occur
- Another JAK-inhibitor has increased the risk of thrombosis, including deep venous thrombosis (DVT), pulmonary embolism (PE), and arterial thrombosis (compared to those treated with TNF blockers) in patients with rheumatoid arthritis, a condition for which Jakafi is not indicated. In patients with myelofibrosis (MF) and polycythemia vera (PV) treated with Jakafi in clinical trials, the rates of thromboembolic events were similar in Jakafi and control treated patients. Patients with symptoms of thrombosis should be promptly evaluated and treated appropriately
- Another JAK-inhibitor has increased the risk of lymphoma and other malignancies excluding NMSC (compared to those treated with TNF blockers) in patients with rheumatoid arthritis, a condition for which Jakafi is not indicated. Patients who are current or past smokers are at additional increased risk. Consider the benefits and risks for the individual patient prior to initiating or continuing therapy with Jakafi, particularly in patients with a known secondary malignancy (other than a successfully treated NMSC), patients who develop a malignancy, and patients who are current or past smokers
- In myelofibrosis and polycythemia vera, the most common nonhematologic adverse reactions (incidence ≥15%) were bruising, dizziness, headache, and diarrhea. In acute graft-versus-host disease, the most common nonhematologic adverse reactions (incidence >50%) were infections (pathogen not specified) and edema. In chronic graft-versus-host disease, the most common nonhematologic adverse reactions (incidence >20%) were infections (pathogen not specified) and viral infections
- Avoid concomitant use with fluconazole doses greater than 200 mg. Dose modifications may be required when administering Jakafi with fluconazole doses of 200 mg or less, or with strong CYP3A4 inhibitors, or in patients with renal or hepatic impairment. Patients should be closely monitored and the dose titrated based on safety and efficacy
- Use of Jakafi during pregnancy is not recommended and should only be used if the potential benefit justifies the potential risk to the fetus. Women taking Jakafi should not breastfeed during treatment and for 2 weeks after the final dose
Please see Full Prescribing Information for Jakafi.